Bioimpacts. 2025;15:30532.
doi: 10.34172/bi.30532
Systematic Review
A systematic review on the use of phytotherapy in managing clinical depression
Sutude Fazilat Conceptualization, Writing – original draft, 1, 2 
Fateme Tahmasbi Writing – review & editing, 3, 4
Mohammad Reza Mirzaei Writing – review & editing, 2
Sarvin Sanaie Methodology, 5
Zahra Yousefi Methodology, 6
Solmaz Asnaashari Writing – review & editing, 7
Shadi Yaqoubi Methodology, 8
Ahad Banagozar Mohammadi Methodology, Supervision, 2, *
Mostafa Araj-khodaei Conceptualization, Supervision, Writing – original draft, 5, *
Author information:
1Research Center for Integrative Medicine in Aging, Aging Research Institute, Tabriz University of Medical Sciences, Tabriz, Iran
2Department of Persian Medicine, Faculty of Traditional Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
3Social Determinants of Health Research Center, Health Management and Safety Promotion Research Institute, Tabriz University of Medical Sciences, Tabriz, Iran
4Research Center for Evidence-based Medicine Iranian EBM Centre: A Joanna Briggs Institute (JBI) Center of Excellence, Tabriz University of Medical Sciences, Tabriz, Iran
5Neurosciences Research Center, Aging Research Institute, Tabriz University of Medical Sciences, Tabriz, Iran
6Research Center of Psychiatry and Behavioral Sciences, Aging Research Institute, Tabriz University of Medical Sciences, Tabriz, Iran
7Biotechnology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
8Faculty of pharmacy, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
The use of medicinal plants in the management of depression, also known as phytotherapy or herbal medicine for depression, is an area of growing interest in the field of mental health and complementary medicine.
Methods:
This study used a systematic assessment of pertinent literature to assess the effectiveness of medicinal herbs in treating mild to severe depression. A comprehensive literature search was conducted to identify randomized controlled trials (RCTs) that reported data on the intervention, control group, adverse events, outcome measurements, and main findings. A summary and analysis were done on the included research data.
Results:
We included 23 RCTs investigating the efficacy of herbal medicines, including Crocus sativus, Lavandula angustifolia, Melissa officinalis, and Echium amoenum, in treating depression. In general, saffron showed encouraging outcomes when used to treat mild to severe depression. With no discernible variations in the reported adverse effects, it proved to be equally efficacious as well-known antidepressants like imipramine and fluoxetine. However, it is noteworthy that not all trials yielded favorable results.
Conclusion:
More investigation is required to fully understand the mechanisms of action, ideal dosage schedules, long-term effects, and relative efficacy of medicinal plants in depressive treatment.
Keywords: Phytotherapy, Herbal medicine, Depression, Depressive disorder, Systematic review
Copyright and License Information
© 2025 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Introduction
Depression is a prevalent mental health condition marked by enduring sadness, despair, and disinterest in activities.1-3 The World Health Organization (WHO) states that depression affects people of all ages and backgrounds and is one of the significant causes of disability globally.4,5 The epidemiology of depression is characterized by an increasing prevalence globally, with estimates suggesting that over 264 million people are affected by depression.6 The burden of depression extends beyond individual suffering to impact families, communities, and societies at large.7 Factors such as socioeconomic status, gender, age, genetics, and environmental stressors can influence the risk of developing depression.8 Contemporary medicine plays a crucial role in managing depression and provides evidence-based treatments, personalized care, monitoring and follow-up, access to specialized services, and technology integration for patient support.9-12 By leveraging the advances in contemporary medicine, healthcare providers can help individuals with depression achieve better outcomes and lead healthier, more fulfilling lives. Phytotherapy, also known as herbal or botanical medicine, is integral to contemporary medicine. It involves the use of plants and plant extracts to prevent, treat, and manage various health conditions, including mental health disorders like depression.13 Many cultures have a long history of using medicinal plants to treat various ailments, including mental health conditions like depression.14 Certain herbs and plants are frequently used in traditional medical systems, including Ayurveda, Traditional Chinese Medicine, and Indigenous healing methods, to treat mood problems. Some medicinal plants contain bioactive compounds that may influence neurotransmitter levels, neuroinflammation, oxidative stress, and other depression-related pathways.15 For instance, it's thought that St. John's Wort (Hypericum perforatum), like other antidepressants, modifies serotonin levels.16 Research studies have investigated the efficacy and safety of certain medicinal plants in treating depression. Herbs like Saffron (Crocus sativus), Rhodiola (Rhodiola rosea), and Ashwagandha (Withania somnifera) have shown promising results in clinical trials for improving depressive symptoms.17,18 While herbal remedies are generally considered safe when used appropriately, it is essential to consider potential side effects, drug interactions, and contraindications. Some herbs may cause adverse reactions or interact with psychiatric medications, highlighting the importance of consulting a healthcare provider before using them. Systematic reviews comprehensively summarize existing research on a specific topic by systematically identifying, appraising, and synthesizing relevant studies. A systematic review can assist in compiling information on the effectiveness, safety, and mechanisms of action of different herbal therapies when it comes to medicinal plants for depression. By critically evaluating the methodological quality and risk of bias in individual studies, a systematic review can assess the overall strength of the evidence supporting the use of medicinal plants for depression. This method assists in identifying areas that require more investigation, discrepancies in the findings, and knowledge gaps. Therefore, our goal was to provide a thorough analysis of the body of research on the use of herbal medicine to treat depression.
Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement was followed in conducting this systematic review.19
Search strategy
An electronic database (PubMed) searches for and reviews the available evidence. The search time was until October 2023. Boolean operators and combinations of keywords were used to find relevant studies. The key terms used for the search include the following: Major depressive disorder, Depression, Depressive Disorder, Melancholia, Dysthymia, Mood disorder, Affective disorder, scientific names, and common names of the medical plants. The medicinal plants mentioned by Ibn Sina in the Canon of Medicine for depression, which he referred to as Mofarrehat, were collected. The list of these plants is detailed in Table 1.
Table 1.
Names of plants as Mofarrehat in the Canon of Medicine
|
Scientific name
|
Family
|
Name in Persian medicine
|
|
Albizzia julibrissin L.
|
Leguminosae |
Abrisham |
|
Centaurea behen L.
|
Compositae |
Bahman |
|
Cinnamomum zeylanicum L. |
Lauraceae |
Darsini |
|
Cinnamomum camphora J.Presl |
Lauraceae |
Kaphour |
|
Cinnamomum cassia J.Presl |
Lauraceae |
Sazej |
|
Citrus media L. |
Rutaceae |
Utruj |
|
Corallium rubrum
|
Corallidae |
Bosd |
|
Coriandrum sativum L. |
Apiaceae |
Kozboreh |
|
Crocus sativus L. |
Iridaceae |
Saffron |
|
Curcuma zedoaria (christm)Roscoe |
Zingiberaceae |
Jadvar |
|
Cyperus longus L. |
Cyperaceae |
Soud |
|
Doronicum pardalianches L. |
Compositae |
Durunaj |
|
Echium amoenum Fisch & C.A.Mey |
Boraginaceae |
Lesan-Al-Sour |
|
Elettaria cardamomum Maton. |
Zingiberaceae |
Gagoleh |
|
Ficus carica L. |
Moraceae |
Teen |
|
Hyacinthus orientalis L. |
Asparagaceae |
Sunbul |
|
Inula helenium L. |
Compositae |
Rasen |
|
Lavandula angustifilia Mill |
Lamiaceae |
Ustokhodus |
|
Malus domestica Borkh |
Rosaceae |
Tofah |
|
Melissa officinalis L. |
Lamiaceae |
Badranjbuyeh |
|
Ocimum basilicum L. |
Lamiaceae |
Badruj |
|
Phyllanthus emblica L. |
Phyllanthuceae |
Amole |
|
Pistacia vera L. |
Anacardiaceae |
Festeg |
|
Polypodium vulgare L. |
Polypodiaceae |
Basfayej |
Polyporus officinalis
Laricifomes officinalis
|
Fomitopsidaceae |
Garigon |
|
Saccharum officinarum L. |
Poaceae |
Tabashir |
|
Santalum album L. |
Santalaceae |
Sandal |
|
Taxus Baccata L. |
Taxaceae |
Zarnub |
|
Terminalia chebula Retz |
Combretaceae |
Halilaj |
|
Zingiber zerumbet Roscoe ex Sm |
Zingiberaceae |
Zoronbad |
Inclusion and exclusion criteria
Studies were included if they met the following conditions: 1) Human randomized clinical trial; 2) Individuals who are diagnosed with depression with no age or gender limitation; 3) The intervention involves the use of the plant in the oral form of a drug. Excluded studies: used another study design (e.g., observational), were another publication type (e.g., systematic reviews), used another intervention or type of drug, investigated combinations of herbs, and were published in a language other than English.
Data extraction
Two members independently reviewed the studies in the first stage according to the abstract and title and, if necessary, used the articles' full text. In case of disagreement, the judgment was made by a third person. Using a Microsoft Excel spreadsheet, two reviewers independently extracted study-related data, including the author's name, year of publication, origin, sample size, outcome measurement tools, intervention type, dosage, duration of use, and other detailed information.
Quality assessment
The quality of studies was evaluated using the Cochrane risk of bias (RoB) assessment tool.20 The Cochrane RoB assessment tool consists of several domains or criteria commonly associated with biases in research studies. These domains typically include: 1. Selection Bias: This domain assesses the methods used to select participants and assign them to different study groups, such as random sequence generation and allocation concealment. 2. Performance Bias: This domain evaluates whether participants and researchers knew the interventions being administered, which could influence outcomes or introduce bias. 3. Detection Bias: This domain examines how outcomes were assessed and whether there was blinding of outcome assessors to minimize bias. 4. Attrition Bias: This domain considers the completeness of outcome data and whether missing data or dropouts could impact the results. 5. Reporting Bias: This domain focuses on selective reporting of outcomes or analyses, which can distort the interpretation of study findings. 6. Other Sources of Bias: This area includes other possible sources of bias not addressed by the preceding domains, such as funding sources, conflicts of interest, or protocol violations in the study.20
Data synthesis
A meta-analysis was neither appropriate nor practicable because of the significant heterogeneity in the included studies. The studies varied significantly in terms of intervention and population. As a result, pooling the data for quantitative synthesis was deemed inappropriate, and a narrative synthesis of the findings was conducted instead.
Results
Literature search
A total of 670 records were identified through the databases. According to the study type, 325 articles were excluded. Moreover, 345 studies were selected for screening. After removing the duplicate studies unrelated to the subject, one hundred and twenty-eight essays remained. One hundred five full-text articles were excluded for the following reasons: The study participants had diseases other than depression or did not have major depressive disorder criteria at the beginning of the clinical trial (n = 37). Studies whose type of intervention was different than the oral method (for example, aromatherapy and topical) (n = 32) study had a non-pharmacological intervention (n = 23), and studies that investigated the effect of a combination of herbs, at least two herbs (n = 13) The final number of 23 RCTs were selected for this review.21-43 Fig. 1 presents a flowchart that illustrates choosing studies.
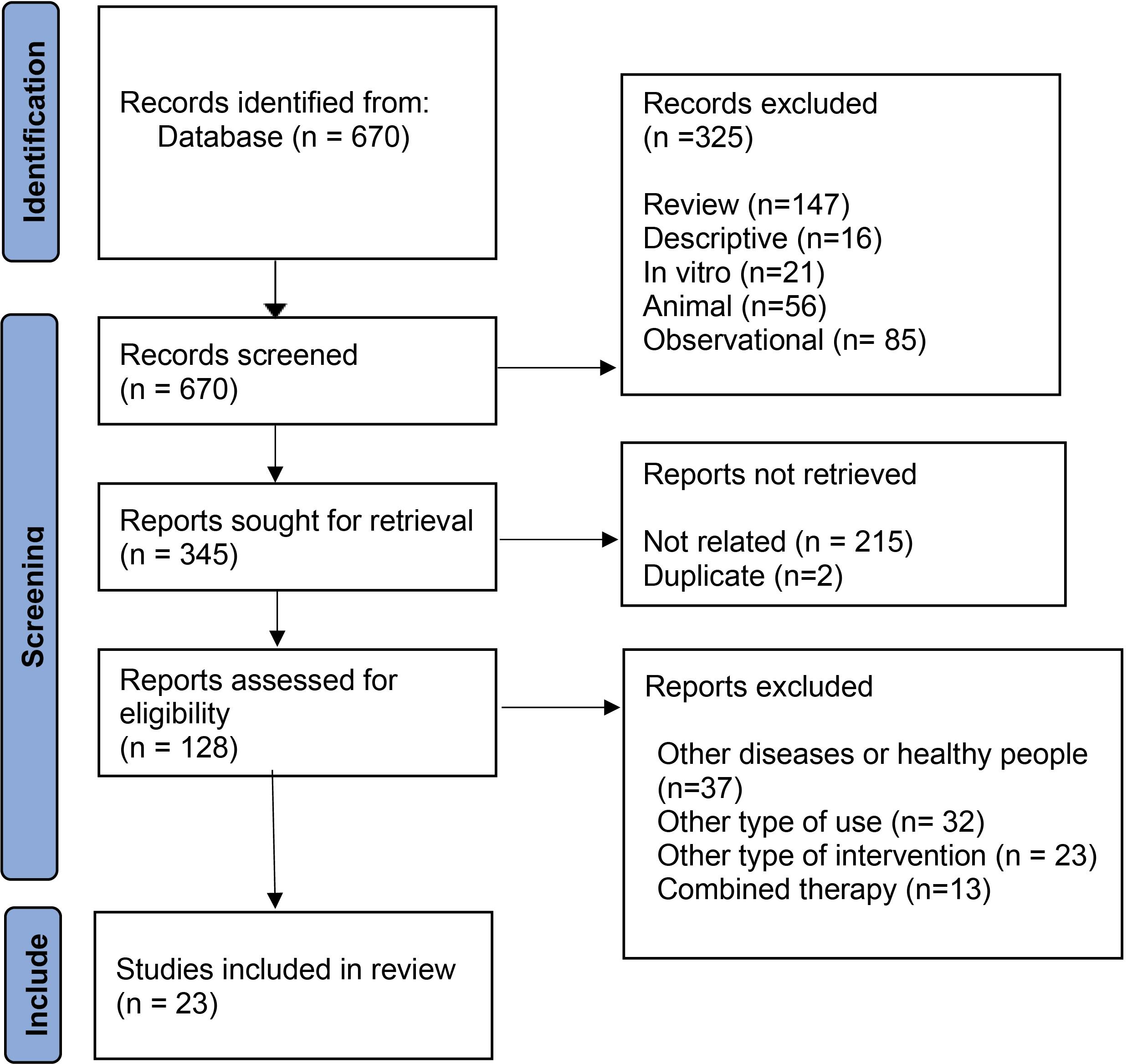
Fig. 1.
Study flow diagram.
.
Study flow diagram.
Study characteristics
Table S1 displays the characteristics of the 23 RCTs that are included. Included studies investigated the effects of phytotherapy, specifically saffron (Crocus sativus), in the treatment of depression. While all the included studies were RCTs, they differ in binding, having a placebo arm or a parallel group. The studies primarily focus on individuals with mild to moderate depression, although some also include patients with postpartum depression,29,42 or depression related to specific conditions like percutaneous coronary intervention (PCI).41 In addition, depression in type 2 diabetes patients was addressed by some studies.34,38
Interventions
It's important to note that the interventions' specific dosages, frequencies, and durations vary across studies. In the majority of the RCTs, the experimental group received saffron capsules. The dosage varied between 30 mg to 50 mg/d, and the duration of intervention ranged from 4 weeks to 12 weeks. Saffron capsules were administered either once daily (OD), twice daily (BD), or three times daily (TDS). In the Akhondzadeh et al study, the control group received imipramine capsules at 100 mg daily (TDS) for 6 weeks.22 In several studies, including Noorbala et al, Moshiri et al, Talaei 2015, and Sahraian et al, the control group received fluoxetine capsules at 20 mg/d (BD) or 40 mg daily for 6 weeks.35,37,39,43 The control group in the Moshiri et al study received placebo capsules twice daily (BD) for 6 weeks. Placebo capsules contain inactive substances and serve as a comparison to evaluate the effects of the active intervention.35 In the Talaei 2015 study, the intervention group received one of the selective serotonin reuptake inhibitors (SSRIs), either sertraline or citalopram, in addition to a crocin tablet.43 The dosages were 50 mg/d for sertraline or 20 mg/d for citalopram, alongside a crocin tablet at a dosage of 30 mg/d (15 mg twice daily) for a duration of 4 weeks.43 In the Sahraian et al study, the experimental group received saffron capsules in combination with 20 mg of fluoxetine daily for 4 weeks.39 In the Ghajar et al study, the intervention group received one of the SSRIs (citalopram, fluoxetine, or sertraline) along with placebo tablets twice daily (BID) for 4 weeks.27 Aside from saffron, use of other phythotherapeutic agents were investigated through other RCTs, including Lavandula angustifolia,23,26,30,36 Melissa officinalis,26,38 and Echium amoenum.40
Outcome measures
In order to evaluate how effectively the treatments worked in lowering depressed symptoms and enhancing general mental health, several outcome measures were employed. The choice of outcome measures may vary across included RCTs. Based on the frequency with which these tools were used, they will be addressed in the following paragraphs.
A. Hamilton Depression Rating Scale (HDRS): The HDRS consists of several items related to mood, sleep, anxiety, weight loss, and other symptoms of depression. The scale is scored based on the presence and severity of symptoms, with higher scores indicating more severe depression.21-23,25-27,29,35-37,40,41
B. Beck Depression Inventory (BDI): This is a self-report tool that gauges how severe depression symptoms are. It consists of multiple items assessing various aspects of depression, including mood, guilt, irritability, and physical symptoms. Based on their experiences throughout the last two weeks, participants rank each item, and the total score on the BDI indicates the level of depressive symptoms, with higher scores indicating more severe depression.24,28,33,39,43
C. Beck Depression Inventory-II (BDI-II): The BDI-II is a self-report questionnaire designed to measure depression severity, much like the BDI. It contains things about physical, emotional, and cognitive symptoms of depression. The total score on the BDI-II indicates the severity of depressive symptoms.38,42
Further details on the study measures are available in Table S1 (see Supplementary file 1).
Therapeutic effects
Based on the information in the table, the studies suggest that saffron (Crocus sativus) may have therapeutic effects in managing depression. The main therapeutic effect observed in the studies is reducing depressive symptoms. Participants who received saffron intervention showed improvements in their depressive symptoms compared to baseline and/or the control groups. The reduction in symptoms was assessed using rating scales such as the HDRS, BDI, and BDI-II. According to specific research, saffron can be just as beneficial as prescription antidepressants, such as fluoxetine or imipramine. The saffron intervention showed comparable or similar reductions in depressive symptoms compared to the control groups receiving these medications. This suggests that saffron may have a similar therapeutic impact on depression as conventional antidepressants. Some studies investigated the use of saffron as an adjunctive therapy alongside standard antidepressant medications like fluoxetine, sertraline, or citalopram. The results indicated that the combination of saffron with these medications may have additional benefits in reducing depressive symptoms compared to medication alone.
Safety profile
The reported side effects in the studies. Here are the common side effects that were mentioned:
-
Anxiety: Reported in multiple studies, including Akhondzadeh et al, Noorbala et al, and Moshiri et al.22,35,37
-
Change in appetite: Reported in multiple studies, including Akhondzadeh et al, Noorbala et al, Moshiri et al, and Ghajar et al.22,27,35,37
-
Nausea: Reported in multiple studies, including Akhondzadeh et al, Moshiri et al, Talaei 2015, and Ghajar et al.22,27,35,43
-
Headache: Reported in multiple studies, including Akhondzadeh et al, Noorbala et al, Moshiri et al, and Ghajar et al.22,27,35,37,43
-
Sedation: Reported in studies like Noorbala et al and Ghajar et al.27,37
-
Dry mouth: Reported in Akhondzadeh et al.22
-
Hypomania: Reported in Akhondzadeh et al and Moshiri et al.22,35
-
Constipation: Reported in Akhondzadeh et al and Moshiri et al.22,35
-
Urinary retention: Reported in Akhondzadeh et al.22
-
Stomach pain: Reported in Moshiri et al.35
-
Tremor: Reported in Moshiri et al.35
-
Sweating: Reported in Moshiri et al.35
-
Heart pounding: Reported in Moshiri et al.35
-
Menometrorrhagia: Reported in Sahraian et al.39
-
Dyspnea: Reported in Sahraian et al.39
-
Agitation: Reported in Sahraian et al.39
-
Morning drowsiness: Reported in Shahmansouri 2014.41
-
Decreased appetite: Reported in Shahmansouri 2014.41
-
Vomiting: Reported in Ghajar et al.27
Methodological quality
Based on the Cochrane risk of bias tool, one study in random sequence generation and three studies in allocation concealment were high risk. Two studies did not explain how participants were blinded. One study specified Detection bias as high risk, but it was unclear in four studies. Attrition bias was determined as high risk in six studies, unclear in one study, and low risk in the remaining studies. Regarding reporting bias, one study was specified as high risk because of incomplete reporting of outcome data, and four studies were classified as unclear. Fig. 2 and Fig. 3 show the risk of bias summary and risk of bias graft respectively.
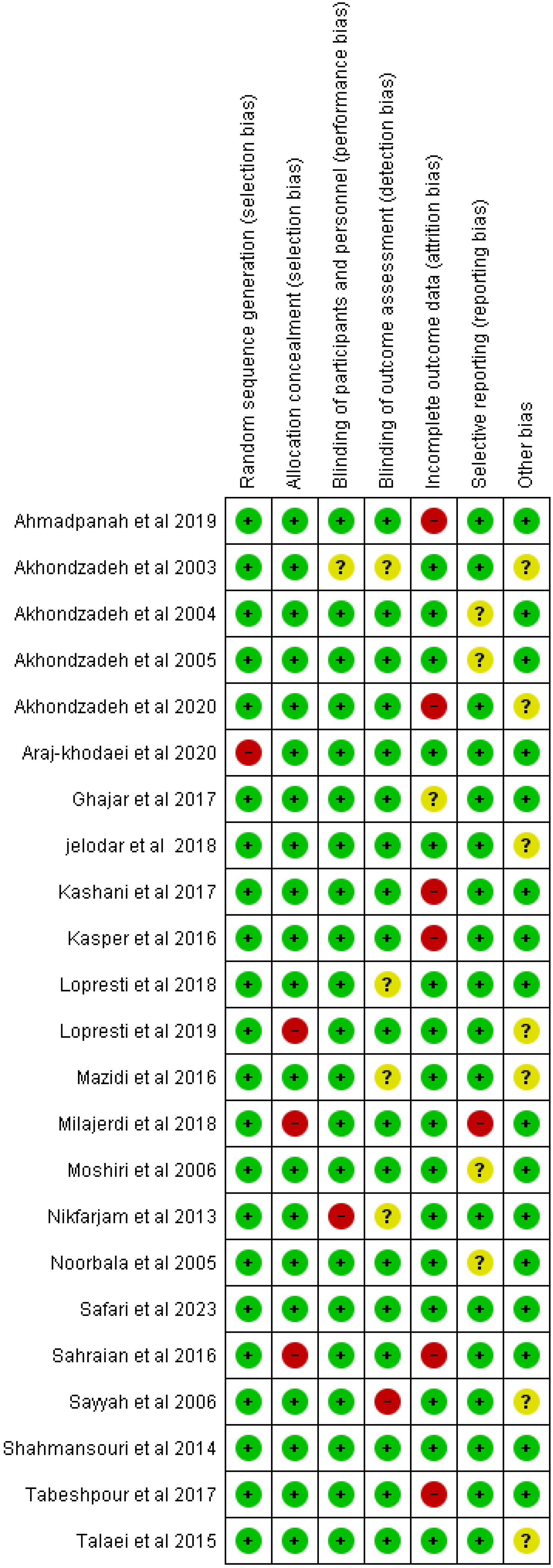
Fig. 2.
Risk of bias summary.
.
Risk of bias summary.
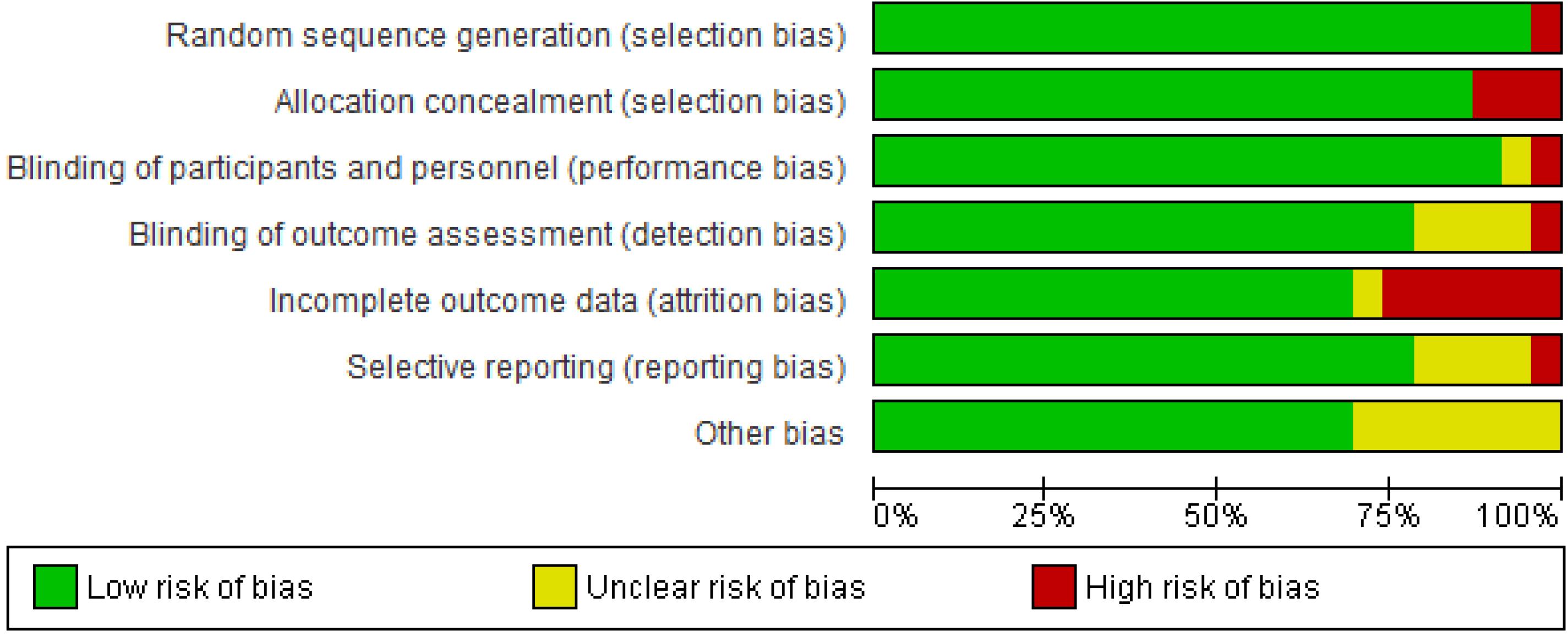
Fig. 3.
Risk of bias graph.
.
Risk of bias graph.
Discussion
Depression is a prevalent mental health disorder that poses significant challenges in terms of effective treatment and management. While conventional pharmacological approaches, such as antidepressant medications and psychotherapy, are commonly utilized, there is growing interest in exploring alternative treatment options, including phytotherapy.44-46 This systematic review aimed to evaluate the use of phytotherapy in the management of depression, with a particular focus on the effectiveness and safety of herbal interventions. The included studies primarily focused on the use of Crocus sativus (saffron) as an herbal intervention for depression. Saffron showed encouraging therapeutic benefits, reducing depression symptoms in a way that was on par with typical antidepressant drugs like imipramine and fluoxetine. These results suggest that saffron may be a viable alternative or adjunctive treatment option for individuals with depression. Moreover, saffron was generally well-tolerated, with only mild and transient side effects reported. This favorable safety profile is encouraging, as it suggests that saffron may provide a potentially safer option compared to some conventional antidepressant medications, which can be associated with side effects and tolerability issues.47 However, it is essential to note that the studies reviewed had relatively small sample sizes and varied dosages and treatment durations, warranting caution in generalizing the findings. Another central point to discuss is that patients with depressive symptoms may prefer phytotherapeutic approaches over conventional treatments for several reasons. For instance, phytotherapeutic approaches often involve using natural herbs and plants, which some patients may find more appealing than synthetic medications. They may feel that a holistic approach that addresses their mental health through natural remedies aligns more with their values and beliefs.48 Also, many conventional antidepressant medications can have significant side effects, such as weight gain, sexual dysfunction, and insomnia.49 Patients may be drawn to phytotherapeutic treatments because they are perceived to have fewer side effects and be gentler on the body.50 While scientific evidence supporting the effectiveness of phytotherapeutic treatments for depression is limited, some patients may believe that these natural remedies are just as effective as conventional medications. Placebo effects and the power of belief can also affect how patients perceive the effectiveness of different treatment approaches.51,52 Therefore, the present review clearly emphasizes the necessity of more study in this area. In addition, although phytotherapy has been getting more recognition worldwide as a complementary and alternative medicine to treat depression, the underlying mechanism of its effectiveness is not well understood yet. When it comes to depression symptoms, several mechanisms are believed to be involved in how phytotherapy can help:
-
Neurotransmitter modulation: Some herbs used in phytotherapy for depression, such as St. John's Wort, may act on neurotransmitters like serotonin, dopamine, and norepinephrine. These herbs can help regulate these neurotransmitters, which are essential for mood regulation.53
-
Anti-inflammatory effects: Chronic inflammation has been linked to depression, and some herbal remedies have anti-inflammatory properties. By reducing inflammation in the body, these herbs may help alleviate depressive symptoms.54
-
Antioxidant effects: Oxidative stress is another factor that can contribute to depression. Certain antioxidant-rich herbs may lessen oxidative stress and shield brain tissue from harm, which may elevate mood.55
-
Adaptogenic effects: Adaptogens are a class of herbs that help the body adapt to stress and maintain balance. Adaptogenic herbs can strengthen resistance to depressive symptoms and lessen the adverse effects of stress on mental health by assisting the body's stress response system.56
-
Anxiolytic effects: Some herbs used in phytotherapy have calming and anxiety-reducing effects, which can be beneficial for individuals experiencing symptoms of anxiety along with depression. These herbs may help improve overall mood by promoting relaxation and reducing anxiety.17,54
It's crucial to remember that even while phytotherapy might be a proper adjunctive strategy for treating depressive symptoms, it cannot take the place of expert medical guidance and care. Hence, it's essential to consult with a healthcare provider to develop a comprehensive treatment plan that may include phytotherapy and other interventions such as therapy and medication.
Strengths and limitations
Identifying gaps in the existing literature through a systematic review can help prioritize future research directions, such as conducting well-designed clinical trials, mechanistic studies, or long-term follow-up investigations on promising medicinal plants for depression. This process contributes to advancing the scientific understanding of phytotherapy in mental health. Transparency and Reproducibility: Systematic reviews follow a transparent and reproducible methodology to ensure the reliability and validity of their findings. Another limitation of this systematic review is the inability to perform a meta-analysis due to substantial heterogeneity among the included studies. Significant variability in study designs, populations, interventions, and outcomes across the included studies hindered the ability to synthesize the data quantitatively. As a result, the findings were synthesized narratively, which may limit the precision and generalizability of the conclusions drawn from this review. It is worth noting that this systematic review focused primarily on saffron, and limited information was available on other herbal interventions for depression. Future research should explore the potential of other herbal remedies, such as Lavandula angustifolia (English lavender), St. John's wort, and others, to provide a comprehensive understanding of the efficacy and safety of phytotherapy in depression. Future studies should aim to elucidate the specific pharmacological mechanisms through which saffron exerts its antidepressant effects. Additionally, large-scale randomized controlled trials with standardized protocols are warranted to establish the optimal dosages, treatment durations, and long-term safety profile of saffron in depression management.
Saffron may offer therapeutic advantages and be a viable therapy choice for those with depressive symptoms, according to the systematic review's findings. The studies utilized different study designs, including double-blinded RCTs and placebo-controlled RCTs. Comparable results were seen with saffron and traditional antidepressants such as imipramine and fluoxetine, with no significant differences in terms of observed side effects. It is crucial to remember that not all trials had excellent results, and further investigation is required to thoroughly understand the possible advantages and restrictions of saffron as a depression cure. Overall, for those with mild to severe depression, the results of this systematic review offer early evidence in favor of using saffron as an alternative or complementary treatment.
Conclusion
Medicinal plants are being progressively explored for managing depression through phytotherapy or herbal medicine. Numerous clinical trials evaluated the effectiveness of medicinal herbs in treating depression. Some plants appeared promising in treating depression, comparable to conventional antidepressants. Further studies are required to understand the mechanisms of action, optimum doses, and longer-duration effects.
Research Highlights
What is the current knowledge?
-
Medicinal plants are increasingly being used in the management of depression, known as phytotherapy or herbal medicine for depression.
-
A study assessed the effectiveness of medicinal herbs in treating depression through a systematic review of relevant literature.
What is new here?
-
23 RCTs were included in the study, focusing on herbs like Crocus sativus, Lavandula angustifolia, Melissa officinalis, and Echium amoenum.
-
Not all trials yielded positive results, indicating the need for further research to understand mechanisms of action, optimal dosages, long-term effects, and overall efficacy of medicinal plants in treating depression.
Competing Interests
Authors declare no conflict of interests.
Ethical Statement
All data generated or analyzed during this study are included in this article and the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplementary files
Supplementary file 1 contains Table S1.
(pdf)
Acknowledgements
This study is the result of a Ph.D. thesis in traditional medicine and was financially supported by a grant from Tabriz University of Medical Sciences (Grant No: 69280).
References
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: APA; 2013.
- Ormel J, Kessler RC, Schoevers R. Depression: more treatment but no drop in prevalence: how effective is treatment? And can we do better?. Curr Opin Psychiatry 2019; 32:348-54. doi: 10.1097/yco.0000000000000505 [Crossref] [ Google Scholar]
- Salik I, Marwaha R. Electroconvulsive therapy. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024.
- World Health Organization (WHO). The World Health Report 2001: Mental Health: New Understanding, New Hope. WHO; 2001.
- Ustün TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ. Global burden of depressive disorders in the year 2000. Br J Psychiatry 2004; 184:386-92. doi: 10.1192/bjp.184.5.386 [Crossref] [ Google Scholar]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1545-602. 10.1016/s0140-6736(16)31678-6.
- Lépine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat 2011; 7:3-7. doi: 10.2147/ndt.s19617 [Crossref] [ Google Scholar]
- Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res 2020; 126:134-40. doi: 10.1016/j.jpsychires.2019.08.002 [Crossref] [ Google Scholar]
- Andrews JM, Nemeroff CB. Contemporary management of depression. Am J Med 1994; 97:24S-32S. doi: 10.1016/0002-9343(94)90360-3 [Crossref] [ Google Scholar]
- Tahmasbi F, Mirghafourvand M, Shamekh A, Mahmoodpoor A, Sanaie S. Effects of probiotic supplementation on cognitive function in elderly: a systematic review and meta-analysis. Aging Ment Health 2022; 26:1778-86. doi: 10.1080/13607863.2021.1966743 [Crossref] [ Google Scholar]
- Tahmasbi F, Araj-Khodaei M, Mahmoodpoor A, Sanaie S. Effects of saffron (Crocus sativus L) on anthropometric and cardiometabolic indices in overweight and obese patients: a systematic review and meta-analysis of randomized controlled trials. Phytother Res 2022; 36:3394-414. doi: 10.1002/ptr.7530 [Crossref] [ Google Scholar]
- Sadat Rafiei SK, Abolghasemi S, Frashidi M, Ebrahimi S, Gharei F, Razmkhah Z. Saffron and sleep quality: a systematic review of randomized controlled trials. Nutr Metab Insights 2023; 16:11786388231160317. doi: 10.1177/11786388231160317 [Crossref] [ Google Scholar]
- Sarbandi Farahani M, Bahramsoltani R, Farzaei MH, Abdollahi M, Rahimi R. Plant-derived natural medicines for the management of depression: an overview of mechanisms of action. Rev Neurosci 2015; 26:305-21. doi: 10.1515/revneuro-2014-0058 [Crossref] [ Google Scholar]
- Dobrek L, Głowacka K. Depression and its phytopharmacotherapy—a narrative review. Int J Mol Sci 2023; 24:4772. doi: 10.3390/ijms24054772 [Crossref] [ Google Scholar]
- Liaqat H, Parveen A, Kim SY. Neuroprotective natural products' regulatory effects on depression via gut-brain axis targeting tryptophan. Nutrients 2022; 14:3270. doi: 10.3390/nu14163270 [Crossref] [ Google Scholar]
- Benzie IF, Wachtel-Galor S. Herbal Medicine: Biomolecular and Clinical Aspects. Boca Raton, FL: CRC Press, Taylor & Francis; 2011.
- Yeung KS, Hernandez M, Mao JJ, Haviland I, Gubili J. Herbal medicine for depression and anxiety: a systematic review with assessment of potential psycho-oncologic relevance. Phytother Res 2018; 32:865-91. doi: 10.1002/ptr.6033 [Crossref] [ Google Scholar]
- Sarris J. Herbal medicines in the treatment of psychiatric disorders: 10-year updated review. Phytother Res 2018; 32:1147-62. doi: 10.1002/ptr.6055 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 2021; 88:105906. doi: 10.1016/j.ijsu.2021.105906 [Crossref] [ Google Scholar]
- Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Assessing risk of bias in a randomized trial. In: Cochrane Handbook for Systematic Reviews of Interventions. Wiley; 2019. p. 205-28.
- Ahmadpanah M, Ramezanshams F, Ghaleiha A, Akhondzadeh S, Sadeghi Bahmani D, Brand S. Crocus sativus L (saffron) versus sertraline on symptoms of depression among older people with major depressive disorders-a double-blind, randomized intervention study. Psychiatry Res 2019; 282:112613. doi: 10.1016/j.psychres.2019.112613 [Crossref] [ Google Scholar]
- Akhondzadeh S, Fallah-Pour H, Afkham K, Jamshidi AH, Khalighi-Cigaroudi F. Comparison of Crocus sativus L and imipramine in the treatment of mild to moderate depression: a pilot double-blind randomized trial [ISRCTN45683816]. BMC Complement Altern Med 2004; 4:12. doi: 10.1186/1472-6882-4-12 [Crossref] [ Google Scholar]
- Akhondzadeh S, Kashani L, Fotouhi A, Jarvandi S, Mobaseri M, Moin M. Comparison of Lavandula angustifolia Mill tincture and imipramine in the treatment of mild to moderate depression: a double-blind, randomized trial. Prog Neuropsychopharmacol Biol Psychiatry 2003; 27:123-7. doi: 10.1016/s0278-5846(02)00342-1 [Crossref] [ Google Scholar]
- Akhondzadeh S, Mostafavi SA, Keshavarz SA, Mohammadi MR, Hosseini S, Eshraghian MR. A placebo controlled randomized clinical trial of Crocus sativus L (saffron) on depression and food craving among overweight women with mild to moderate depression. J Clin Pharm Ther 2020; 45:134-43. doi: 10.1111/jcpt.13040 [Crossref] [ Google Scholar]
- Akhondzadeh S, Tahmacebi-Pour N, Noorbala AA, Amini H, Fallah-Pour H, Jamshidi AH. Crocus sativus L in the treatment of mild to moderate depression: a double-blind, randomized and placebo-controlled trial. Phytother Res 2005; 19:148-51. doi: 10.1002/ptr.1647 [Crossref] [ Google Scholar]
- Araj-Khodaei M, Noorbala AA, Yarani R, Emadi F, Emaratkar E, Faghihzadeh S. A double-blind, randomized pilot study for comparison of Melissa officinalis L and Lavandula angustifolia Mill with fluoxetine for the treatment of depression. BMC Complement Med Ther 2020; 20:207. doi: 10.1186/s12906-020-03003-5 [Crossref] [ Google Scholar]
- Ghajar A, Neishabouri SM, Velayati N, Jahangard L, Matinnia N, Haghighi M. Crocus sativus L versus citalopram in the treatment of major depressive disorder with anxious distress: a double-blind, controlled clinical trial. Pharmacopsychiatry 2017; 50:152-60. doi: 10.1055/s-0042-116159 [Crossref] [ Google Scholar]
- Jelodar G, Javid Z, Sahraian A, Jelodar S. Saffron improved depression and reduced homocysteine level in patients with major depression: a randomized, double-blind study. Avicenna J Phytomed 2018; 8:43-50. [ Google Scholar]
- Kashani L, Eslatmanesh S, Saedi N, Niroomand N, Ebrahimi M, Hosseinian M. Comparison of saffron versus fluoxetine in treatment of mild to moderate postpartum depression: a double-blind, randomized clinical trial. Pharmacopsychiatry 2017; 50:64-8. doi: 10.1055/s-0042-115306 [Crossref] [ Google Scholar]
- Kasper S, Volz HP, Dienel A, Schläfke S. Efficacy of Silexan in mixed anxiety-depression--a randomized, placebo-controlled trial. Eur Neuropsychopharmacol 2016; 26:331-40. doi: 10.1016/j.euroneuro.2015.12.002 [Crossref] [ Google Scholar]
- Lopresti AL, Drummond PD, Inarejos-García AM, Prodanov M. affron®, a standardised extract from saffron (Crocus sativus L) for the treatment of youth anxiety and depressive symptoms: a randomised, double-blind, placebo-controlled study. J Affect Disord 2018; 232:349-57. doi: 10.1016/j.jad.2018.02.070 [Crossref] [ Google Scholar]
- Lopresti AL, Smith SJ, Hood SD, Drummond PD. Efficacy of a standardised saffron extract (affron®) as an add-on to antidepressant medication for the treatment of persistent depressive symptoms in adults: a randomised, double-blind, placebo-controlled study. J Psychopharmacol 2019; 33:1415-27. doi: 10.1177/0269881119867703 [Crossref] [ Google Scholar]
- Mazidi M, Shemshian M, Mousavi SH, Norouzy A, Kermani T, Moghiman T. A double-blind, randomized and placebo-controlled trial of saffron (Crocus sativus L) in the treatment of anxiety and depression. J Complement Integr Med 2016; 13:195-9. doi: 10.1515/jcim-2015-0043 [Crossref] [ Google Scholar]
- Milajerdi A, Jazayeri S, Shirzadi E, Hashemzadeh N, Azizgol A, Djazayery A. The effects of alcoholic extract of saffron (Crocus satious L) on mild to moderate comorbid depression-anxiety, sleep quality, and life satisfaction in type 2 diabetes mellitus: a double-blind, randomized and placebo-controlled clinical trial. Complement Ther Med 2018; 41:196-202. doi: 10.1016/j.ctim.2018.09.023 [Crossref] [ Google Scholar]
- Moshiri E, Akhondzadeh Basti A, Noorbala AA, Jamshidi AH, Abbasi SH, Akhondzadeh S. Crocus sativus L (petal) in the treatment of mild-to-moderate depression: a double-blind, randomized and placebo-controlled trial. Phytomedicine 2006; 13:607-11. doi: 10.1016/j.phymed.2006.08.006 [Crossref] [ Google Scholar]
- Nikfarjam M, Parvin N, Assarzadegan N, Asghari S. The effects of Lavandula angustifolia Mill infusion on depression in patients using citalopram: a comparison study. Iran Red Crescent Med J 2013; 15:734-9. doi: 10.5812/ircmj.4173 [Crossref] [ Google Scholar]
- Noorbala AA, Akhondzadeh S, Tahmacebi-Pour N, Jamshidi AH. Hydro-alcoholic extract of Crocus sativus L versus fluoxetine in the treatment of mild to moderate depression: a double-blind, randomized pilot trial. J Ethnopharmacol 2005; 97:281-4. doi: 10.1016/j.jep.2004.11.004 [Crossref] [ Google Scholar]
- Safari M, Asadi A, Aryaeian N, Fallah Huseini H, Shidfar F, Jazayeri S. The effects of Melissa officinalis on depression and anxiety in type 2 diabetes patients with depression: a randomized double-blinded placebo-controlled clinical trial. BMC Complement Med Ther 2023; 23:140. doi: 10.1186/s12906-023-03978-x [Crossref] [ Google Scholar]
- Sahraian A, Jelodar S, Javid Z, Mowla A, Ahmadzadeh L. Study the effects of saffron on depression and lipid profiles: a double-blind comparative study. Asian J Psychiatr 2016; 22:174-6. doi: 10.1016/j.ajp.2015.10.012 [Crossref] [ Google Scholar]
- Sayyah M, Sayyah M, Kamalinejad M. A preliminary randomized double blind clinical trial on the efficacy of aqueous extract of Echium amoenum in the treatment of mild to moderate major depression. Prog Neuropsychopharmacol Biol Psychiatry 2006; 30:166-9. doi: 10.1016/j.pnpbp.2005.10.005 [Crossref] [ Google Scholar]
- Shahmansouri N, Farokhnia M, Abbasi SH, Kassaian SE, Noorbala Tafti AA, Gougol A. A randomized, double-blind, clinical trial comparing the efficacy and safety of Crocus sativus L with fluoxetine for improving mild to moderate depression in post percutaneous coronary intervention patients. J Affect Disord 2014; 155:216-22. doi: 10.1016/j.jad.2013.11.003 [Crossref] [ Google Scholar]
- Tabeshpour J, Sobhani F, Sadjadi SA, Hosseinzadeh H, Mohajeri SA, Rajabi O. A double-blind, randomized, placebo-controlled trial of saffron stigma (Crocus sativus L) in mothers suffering from mild-to-moderate postpartum depression. Phytomedicine 2017; 36:145-52. doi: 10.1016/j.phymed.2017.10.005 [Crossref] [ Google Scholar]
- Talaei A, Hassanpour Moghadam M, Sajadi Tabassi SA, Mohajeri SA. Crocin, the main active saffron constituent, as an adjunctive treatment in major depressive disorder: a randomized, double-blind, placebo-controlled, pilot clinical trial. J Affect Disord 2015; 174:51-6. doi: 10.1016/j.jad.2014.11.035 [Crossref] [ Google Scholar]
- Dobrek L, Głowacka K. Depression and its phytopharmacotherapy-a narrative review. Int J Mol Sci 2023; 24:4772. doi: 10.3390/ijms24054772 [Crossref] [ Google Scholar]
- Burstein O, Shamir A, Abramovitz N, Doron R. Patients' attitudes toward conventional and herbal treatments for depression and anxiety: a cross-sectional Israeli survey. Int J Soc Psychiatry 2022; 68:589-99. doi: 10.1177/0020764021992385 [Crossref] [ Google Scholar]
- Haller H, Anheyer D, Cramer H, Dobos G. Complementary therapies for clinical depression: an overview of systematic reviews. BMJ Open 2019; 9:e028527. doi: 10.1136/bmjopen-2018-028527 [Crossref] [ Google Scholar]
- Siddiqui MJ, Saleh MS, Basharuddin S, Zamri SH, Mohd Najib MH, Che Ibrahim MZ. Saffron (Crocus sativus L): as an antidepressant. J Pharm Bioallied Sci 2018; 10:173-80. doi: 10.4103/jpbs.jpbs_83_18 [Crossref] [ Google Scholar]
- Gureje O, Nortje G, Makanjuola V, Oladeji B, Seedat S, Jenkins R. The role of global traditional and complementary systems of medicine in treating mental health problems. Lancet Psychiatry 2015; 2:168-77. doi: 10.1016/s2215-0366(15)00013-9 [Crossref] [ Google Scholar]
- Ferguson JM. SSRI antidepressant medications: adverse effects and tolerability. Prim Care Companion J Clin Psychiatry 2001; 3:22-7. doi: 10.4088/pcc.v03n0105 [Crossref] [ Google Scholar]
- Welz AN, Emberger-Klein A, Menrad K. Why people use herbal medicine: insights from a focus-group study in Germany. BMC Complement Altern Med 2018; 18:92. doi: 10.1186/s12906-018-2160-6 [Crossref] [ Google Scholar]
- Kaptchuk TJ. The placebo effect in alternative medicine: can the performance of a healing ritual have clinical significance?. Ann Intern Med 2002; 136:817-25. doi: 10.7326/0003-4819-136-11-200206040-00011 [Crossref] [ Google Scholar]
- Schulz P, Hede V. Alternative and complementary approaches in psychiatry: beliefs versus evidence. Dialogues Clin Neurosci 2018; 20:207-14. doi: 10.31887/DCNS.2018.20.3/pschulz [Crossref] [ Google Scholar]
- Lee G, Bae H. Therapeutic effects of phytochemicals and medicinal herbs on depression. Biomed Res Int 2017; 2017:6596241. doi: 10.1155/2017/6596241 [Crossref] [ Google Scholar]
- Kenda M, Kočevar Glavač N, Nagy M, Sollner Dolenc M. Medicinal plants used for anxiety, depression, or stress treatment: an update. Molecules 2022; 27:6021. doi: 10.3390/molecules27186021 [Crossref] [ Google Scholar]
- Juszczyk G, Mikulska J, Kasperek K, Pietrzak D, Mrozek W, Herbet M. Chronic stress and oxidative stress as common factors of the pathogenesis of depression and Alzheimer's disease: the role of antioxidants in prevention and treatment. Antioxidants (Basel) 2021; 10:1439. doi: 10.3390/antiox10091439 [Crossref] [ Google Scholar]
- Panossian A, Wikman G. Effects of adaptogens on the central nervous system and the molecular mechanisms associated with their stress-protective activity. Pharmaceuticals (Basel) 2010; 3:188-224. doi: 10.3390/ph3010188 [Crossref] [ Google Scholar]