Bioimpacts. 15:30813.
doi: 10.34172/bi.30813
Original Article
Exploring the potential of tubulin-associated unit protein as a biomarker for schizophrenia
Ali Reza Shafiee-Kandjani Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – review & editing, 1 
Ali Bazzaz Haghighat Talab Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – review & editing, 2
Sara Farhang Conceptualization, Data curation, Resources, Supervision, Writing – review & editing, 1
Dariush Shanehbandi Data curation, Resources, Validation, Writing – review & editing, 3
Milad Asadi Investigation, Methodology, 3
Ailar Nakhlband Investigation, Supervision, Writing – original draft, 4, *
Author information:
1Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran
2Department of Psychiatry, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
3Immunology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
4Research Center for Pharmaceutical Nanotechnology, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Introduction:
Schizophrenia is a chronic and debilitating psychiatric disease characterized by various causes and symptoms. The tau protein is recognized as a biomarker that plays a crucial role in neurocognitive and neurodegenerative diseases. Given the presence of cognitive symptoms in individuals with schizophrenia, the objective of this study was to measure to evaluate the diagnostic potential of measuring serum levels of total tau and phosphorylated tau in patients with schizophrenia.
Methods:
A total of 40 patients with schizophrenia who met the inclusion criteria were selected, along with 40 age- and sex-matched healthy individuals. Written consent was obtained from all participants, and blood samples were collected to measure the serum levels of total tau protein and phosphorylated tau. The obtained data were analyzed using appropriate statistical methods with SPSS 23 software.
Results:
There was no statistically significant disparity detected in the serum concentrations of total and phosphorylated tau protein when comparing individuals with schizophrenia to those without the disorder.
Conclusion:
Based on the results obtained, it can be concluded that total tau protein and phosphorylated tau cannot be considered as diagnostic biomarkers for schizophrenia. Furthermore, the findings of this study do not support the presence of neuroanalysis in schizophrenia.
Keywords: Tubulin associated unit protein, Biomarker, Schizophrenia, Psychiatric disease
Copyright and License Information
© 2025 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This project was conducted as part of a residency thesis of Dr Ali Bazzaz Haghighat Talab approved by Tabriz University of Medical Sciences (code 61834).
Introduction
Schizophrenia is a major psychiatric disorder that places a significant burden on society, affecting approximately 1% of the global population.1 The disorder is characterized by three classes of symptoms: positive symptoms (such as delusions and hallucinations), negative symptoms (including social isolation and decreased productivity), and cognitive impairment symptoms. Numerous studies have found similarities in cognitive impairments between patients with schizophrenia and those with dementia caused by Alzheimer's disease (AD). These studies have shown that hospitalized patients with schizophrenia consistently score lower on cognitive tests (such as the MMSE) compared to control groups, and this decline in scores tends to worsen with age. These findings have led to the hypothesis that the development of neurodegenerative diseases, particularly Alzheimerʹs, as patients age may partially contribute to the observed reduction in MMSE scores.2 It is well-established that in AD and related neurodegenerative disorders, a protein called tau forms insoluble filaments known as neurofibrillary tangles. Tau is a phosphoprotein primarily found in the axons of nerve cells, where its main function is to stabilize microtubule proteins.3 Tau has six major isoforms that are expressed in adult nerve cells. Analysis of the protein's structure has revealed a microtubule-binding domain located at the carboxyl terminus, which consists of repetitive motifs that are fully conserved.4 This region, rich in basic amino acids, plays a crucial role in the formation of tau protein accumulations and the development of intertwined filamentous structures known as PHF. Furthermore, this region is also implicated in the pathology of AD. Tau protein binding to microtubular proteins through phosphorylation/dephosphorylation processes is regulated by specific kinases and phosphatases.5 Abnormal phosphorylation of tau protein in AD leads to the formation of neurofibrillary tangles, indicating the extent of neurofibrillary damage and nerve degeneration.6,7 The volume of these aggregated clumps directly correlates with clinical symptoms, and their deposition sites align with neurological defects in different areas.8,9 Psychotic symptoms have been reported in a significant number of Alzheimer's patients, and these symptoms can exacerbate cognitive complications. The heritability of psychosis in these patients is reported to be 30%.10 Studies have shown an increase in Tau protein and amyloid beta in Alzheimer's patients with psychosis, suggesting an acceleration of neurodegenerative processes.11 Moreover, the concentration of phosphorylated tau (p-tau) in the lateral prefrontal cortex (DLPFC) of Alzheimer's patients increases with psychosis, which is potentially a sign of increased kinase activity resulting in tau phosphorylation.
Despite the importance of schizophrenia, there is currently no specific test or biomarker available for its diagnosis. Early detection and treatment of schizophrenia are crucial in reducing the burden of the disease.12 Finding biomarkers for psychiatric disorders like schizophrenia could lead to more effective treatments and early diagnosis, opening new avenues for preventive and therapeutic approaches.
While there have been studies on the role of tau in dementia, few studies have investigated its role in schizophrenia. In this study, we aimed to assess the levels of tau and phosphorylated tau proteins in the serum of patients with recent-onset schizophrenia compared to a control group. This research aims to contribute to the development of new tools for the accurate diagnosis of schizophrenia.
Materials and Methods
The serum samples of 40 patients with schizophrenia and 40 healthy subjects were obtained from the Azeri Recent Onset/Acute phase psychosis Survey (ARAS) Cohort study. Patients with schizophrenia met the DSM-V diagnostic criteria and were diagnosed through SCID interviews and hospitalized in Razi Hospital, Tabriz University of Medical Sciences.
Cases of acute psychosis, substance-induced psychosis, and mood psychosis were excluded. Participants in the control group were selected through calls sent to local healthcare centers and universities and Razi Hospital in Tabriz, considering their age and sex. The sample size was estimated to be 40 people after applying the inclusion and exclusion criteria by the available sampling method. The control group was matched to the same number of 40 individuals simultaneously, considering age and gender characteristics. Based on the study by Demirel et al,12 with serum levels of tau and p-tau as primary outcomes, an alpha level of 0.05, and a power of 90%, the required sample size was calculated to be 13 patients per group to detect a mean between-group difference of 93.73 points in p-tau levels. This number was determined to be 17 patients for a 149.90-point mean between-group differences for tau levels. Considering a 15% possibility of dropout, a higher sample size of 20 patients per group was recruited for this trial.
Healthy individuals were selected through standard questionnaires, in addition to a clinical interview and detailed history-taking regarding psychiatric diseases, substance use, and other disorders.13 The inclusion criteria for schizophrenia patients were a definitive diagnosis of schizophrenia based on interviews and psychiatric examinations by two assistants and a relevant professor, according to DSM-V criteria and the standard SCID questionnaire. Patients of both genders between the ages of 18-45 were included in the study with their consent.
The exclusion criteria for schizophrenia patients included mood psychosis caused by substances, decomposition disorders, physical diseases, cognitive diseases, and mental retardation. Patients with a history of drug or alcohol use and dependence, as well as those with any infectious or chronic rheumatic disease, were also excluded from the study.
Methods
The present study was non-interventional, and the patients were not deprived of any treatment. The PANSS is a 30-item scale that assesses positive, negative, and general psychopathology symptoms in patients with schizophrenia. Each item is rated on a 7-point scale, with higher scores indicating more severe symptoms. The PANSS has been shown to have good reliability and validity in measuring symptoms of schizophrenia.
Patients and the control group were invited to Razi Hospital in Tabriz for sampling. A blood sample of 2 cc was collected through sterile venipuncture and transferred to a Falcon tube containing 5% EDTA. This sample was then centrifuged at 23 °C for 10 minutes at 1300 rpm. After centrifugation and plasma separation, the sample was subjected to Enzyme-linked immunosorbent assay (ELISA) to measure the serum level of total and phosphorylated tau protein. It is important to note that the samples were stored at -80 °C until the tests were performed. To detect tau protein in the blood samples, an ELISA test was performed by Crystal Day Biotech Co. ELISA kit according to manufacturer protocol.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics 23.0 software. GraphPad Prism version 6.00 software was utilized to generate the graphs. Kolmogorov-Smirnov tests were used to assess the normal distribution of the data. Data are expressed as frequency, median (minimum-maximum), and mean ± standard deviation. To compare total and phosphorylated tau protein in two groups, a t-test was used to model data and draw conclusions. Spearman correlation coefficient was used to compare relative variables and Chi-square test was used to compare nominal variables. A value of P< 0.05 was considered significant.
Results
In the current study, researchers compared the levels of total tau protein and phosphorylated tau protein between 40 patients with schizophrenia and 40 healthy individuals (control group). Both groups consisted of 20 males and 20 females.
The average age of the patient group was 34.85 ± 7.10 years, and that of the control group was 31.03 ± 6.43. The demographic data of the patients and the control group are demonstrated in Table 1.
Table 1.
The demographic findings of the patients and the control group
|
Parameters
|
Patients
|
Controls
|
P
value
|
| Gender (M/F) |
20/20 |
20/20 |
>0.05 |
| Age (years) |
34.85 ± 7.102 |
31.03 ± 6.435 |
>0.05 |
| Marital status (S/ M) |
33/7 |
6/34 |
<0.0001 |
| Employment status (E/U) |
2/38 |
33/7 |
<0.0001 |
| Number of siblings |
2.5 ± 1.3 |
2.05 ± 1 |
>0.05 |
| Duration of marriage (years) |
4.6 (0 – 25) |
5.6 (0–15) |
>0.05 |
| Number of children |
0.52 ± 1 |
0.77 ± 0.8 |
>0.05 |
| Duration of education (years) |
8.3 ± 4.1 |
16.3 ± 2.6 |
<0.0001 |
| Smoker |
17 (42.5%) |
7 (17.5%) |
< 0.05 |
Among the patients, the average time of disease onset was 11.75 ± 5 years, and they had been hospitalized an average of 3.45 times. Ten patients (25%) reported a positive family history of schizophrenia. In terms of medication, 37 patients (92.5%) were using second-generation antipsychotic drugs, 1 patient (2.5%) was using first-generation antipsychotic drugs, and 2 patients (5%) were using a combination of both types. Additionally, 3 patients (7.5%) had a history of receiving electroshock therapy (ECT). The PANSS test was used to assess symptoms in the patient group. The average score for positive symptoms of schizophrenia was 19.05 ± 8, the average score for negative symptoms was 22.1 ± 8, and the score for general symptoms was 31.1 ± 6.8. The specific data for the patient group were summarized in Table 2.
Table 2.
Summary of specific data of the patient group
|
Parameters
|
Values
|
| Disease onset (years) |
11.75 ± 5 |
| Number of hospitalizations |
3.45 ± 2.67 |
| Family history |
10 (25%) |
| Number of previous ECT |
3 (7.5%) |
| Medication |
|
| Atypical antipsychotics |
37 (92.5%) |
| Typical antipsychotics |
1 (2.5%) |
| Both |
2 (5%) |
| PANSS score |
|
| Positive |
19.05 ± 8 |
| Negative |
22.1 ± 8 |
| General |
31.1 ± 6.8 |
To compare the levels of total tau protein and phosphorylated tau protein between the patient and control groups, a Mann-Whitney U test was performed. The results did not show a significant difference in total tau protein levels (P = 0.6965, Mann-Whitney U = 759) or phosphorylated tau protein levels (P = 0.97, Mann-Whitney U = 796.5) between the two groups (Fig. 1).
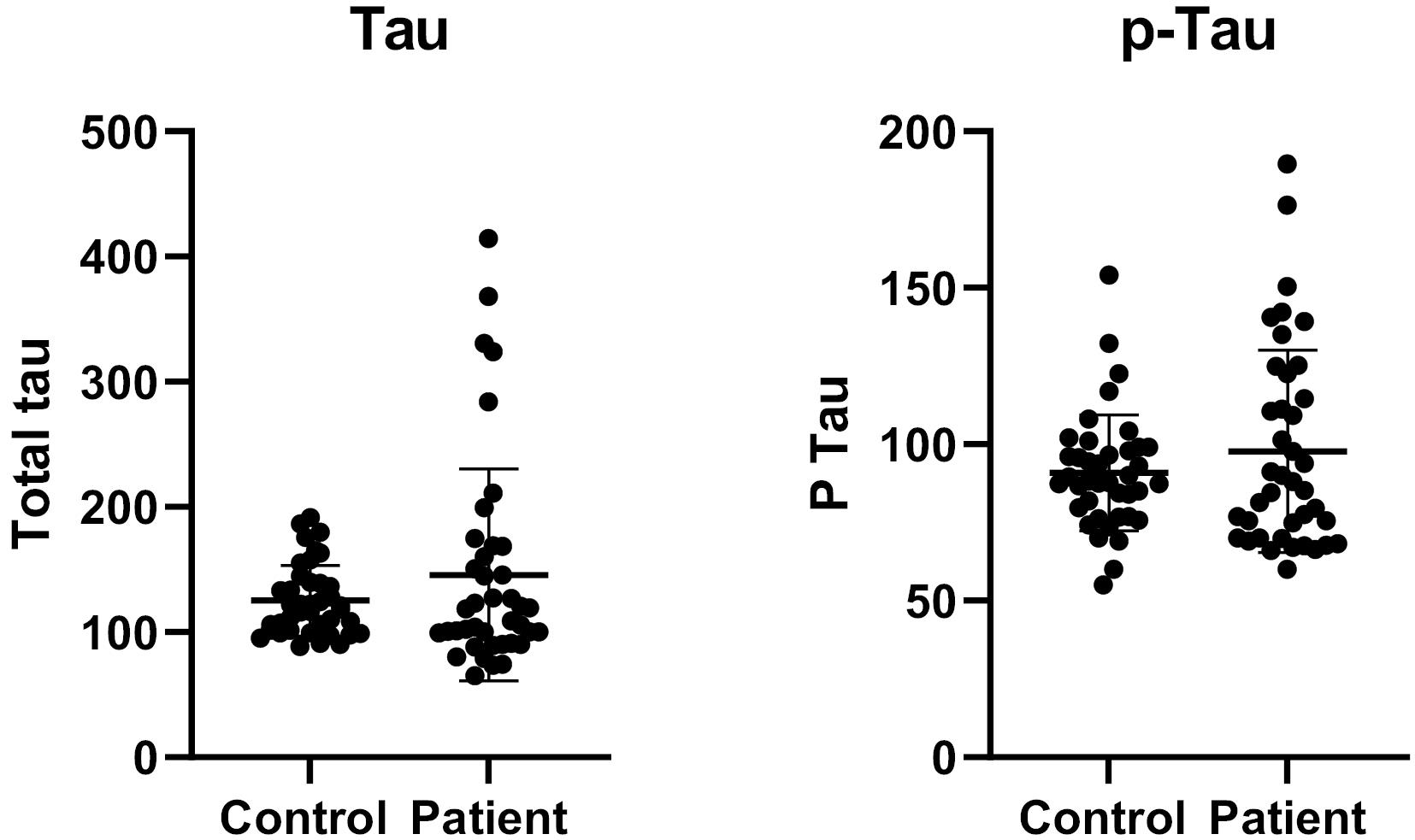
Fig. 1.
Comparison of total tau protein levels (A) and phosphorylated tau protein levels (B) between patient and control groups using the Mann-Whitney U test. No significant differences were observed in total tau (P = 0.6965) or phosphorylated tau (P = 0.97) levels.
.
Comparison of total tau protein levels (A) and phosphorylated tau protein levels (B) between patient and control groups using the Mann-Whitney U test. No significant differences were observed in total tau (P = 0.6965) or phosphorylated tau (P = 0.97) levels.
Furthermore, there was no significant difference in total tau protein levels between males and females or in phosphorylated tau protein levels within the patient group (Fig. 2).
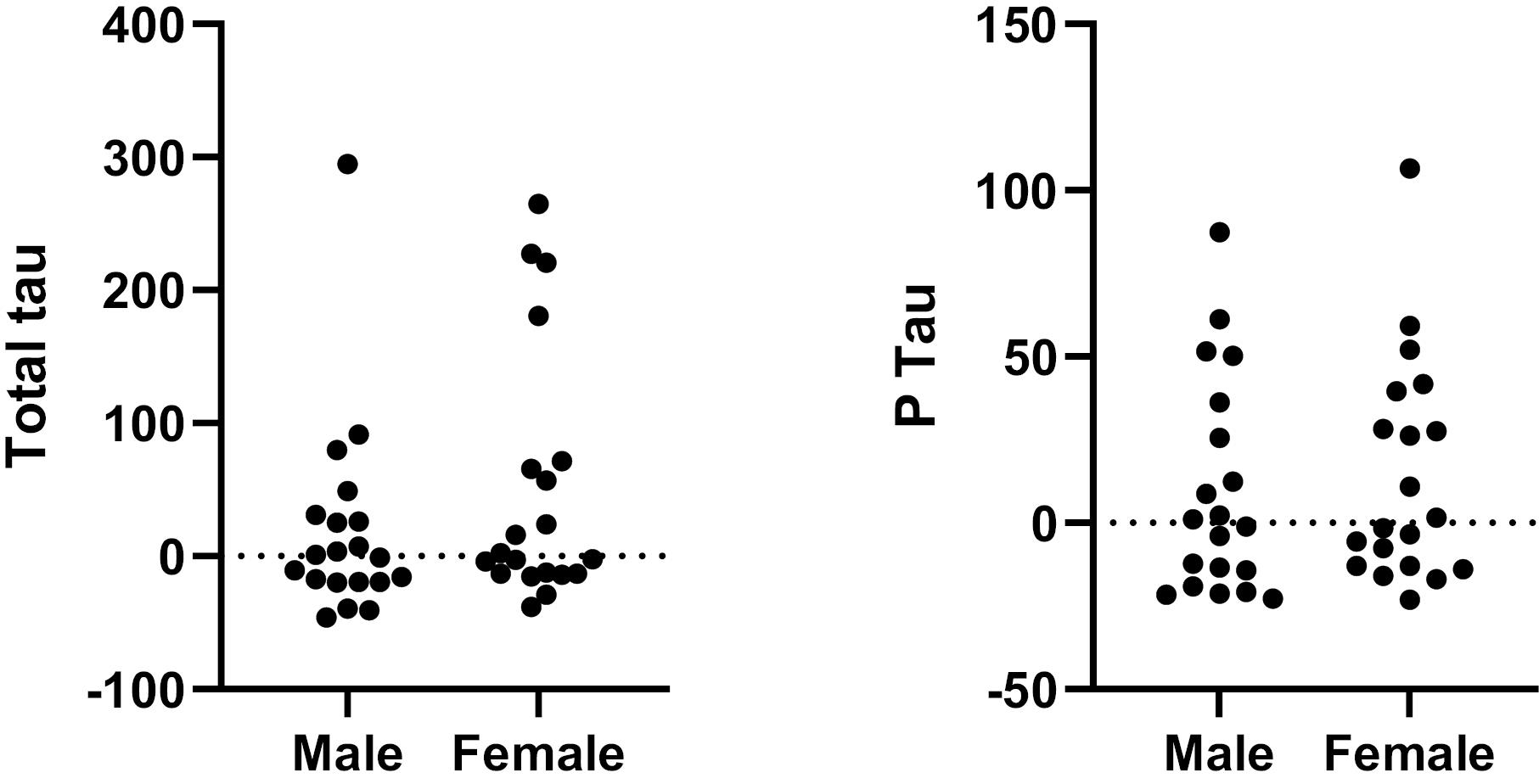
Fig. 2.
Comparison of total tau protein levels (A) and phosphorylated tau protein levels (B) between males and females using the Mann-Whitney U test. No significant difference were observed in total tau protein levels (A) or phosphorylated tau protein levels (B) between males and females within the patient group.
.
Comparison of total tau protein levels (A) and phosphorylated tau protein levels (B) between males and females using the Mann-Whitney U test. No significant difference were observed in total tau protein levels (A) or phosphorylated tau protein levels (B) between males and females within the patient group.
To assess the diagnostic potential of these cytokines as biomarkers, we employed the receiver operating characteristic (ROC) curve analysis. In this method, the area under the curve (AUC) serves as an indicator of the predictive accuracy of total and phosphorylated tau protein levels in distinguishing patients with schizophrenia from healthy controls. An AUC value of 0.5 or lower reflects a lack of diagnostic utility. While a value greater than 0.5 suggests a greater chance for diagnostic value of this biomarker.
Our study found that the AUC value for serum levels of total tau protein was 0.5205 (P = 0.69). Therefore, based on the graphs and the size of the area under the curve, the measurement of total and phosphorylated tau protein levels does not have diagnostic value in distinguishing between patients with schizophrenia and the control group. Linear regression and Spearman's correlation coefficient was used for evaluation of correlations. A significant correlation between total tau protein and phosphorylated tau was observed in patients (Spearman r = 0.81, P value < 0.05) (Fig. 3).
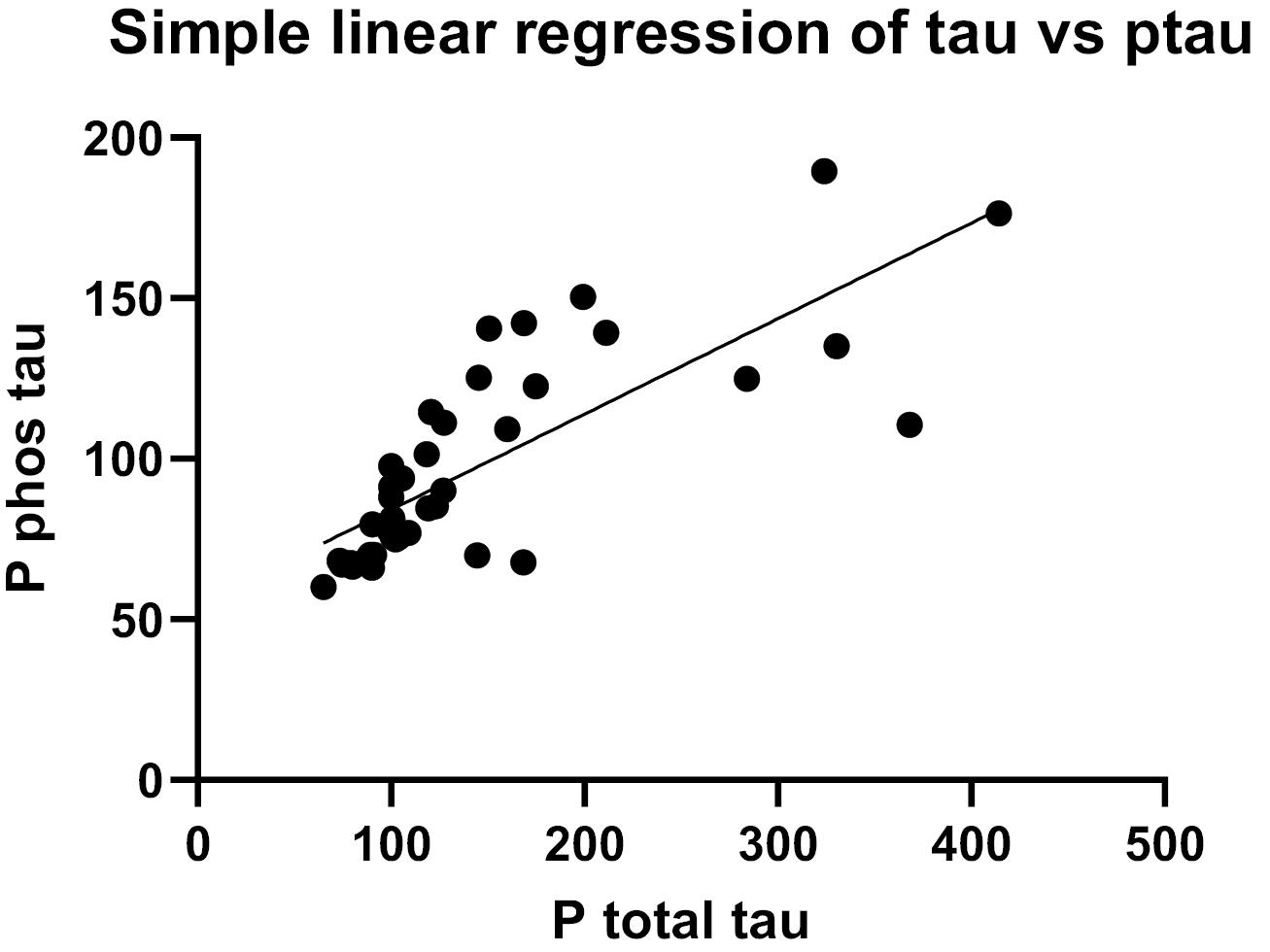
Fig. 3.
Linear regression and Spearman's correlation coefficient were used to assess correlations. A significant positive correlation was observed between total tau and phosphorylated tau in patients (Spearman r = 0.81, P < 0.05).
.
Linear regression and Spearman's correlation coefficient were used to assess correlations. A significant positive correlation was observed between total tau and phosphorylated tau in patients (Spearman r = 0.81, P < 0.05).
Furthermore, significant correlations were found between the age of patients and serum levels of total tau protein (Spearman r = 0.69, P value < 0.05) and phosphorylated tau (Spearman r = 0.57, P value < 0.05). These correlations suggest that the levels of these two proteins increase with age (Fig. 4).
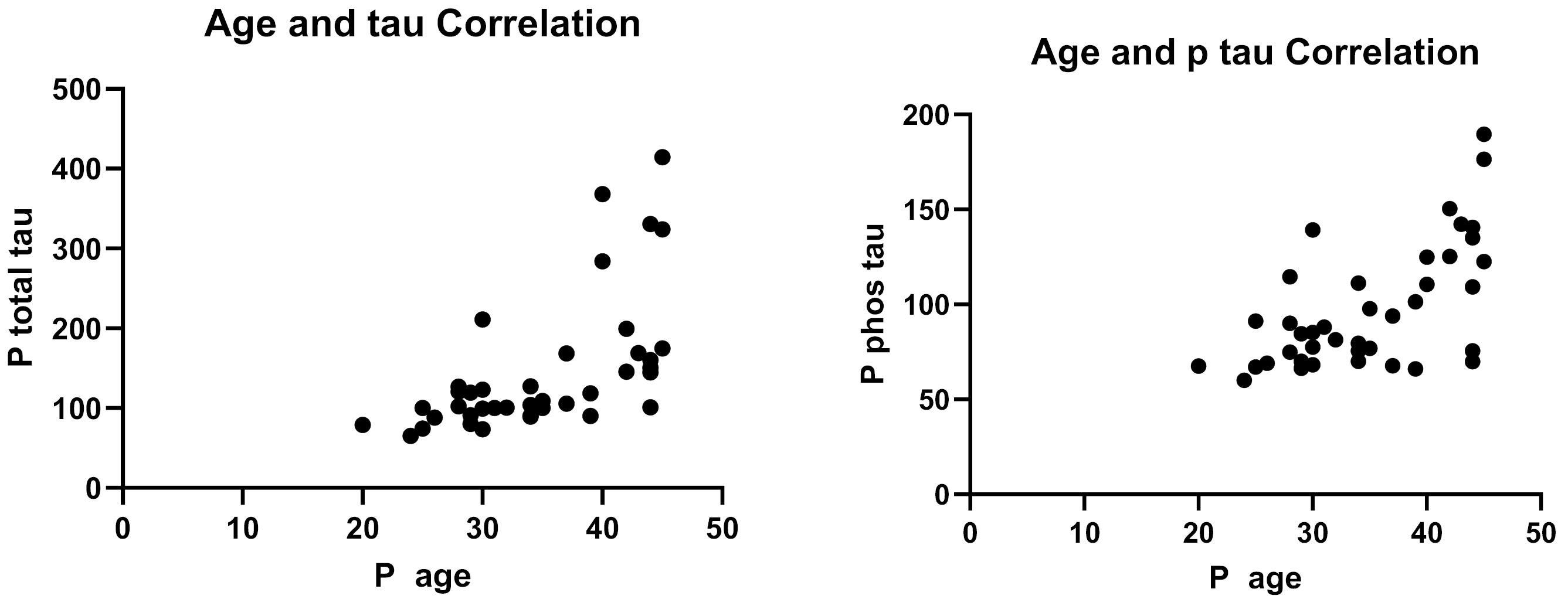
Fig. 4.
Serum levels of total tau (A) and phosphorylated tau (B) show significant positive correlations with patient age (Spearman r = 0.69 and 0.57, respectively; P < 0.05), indicating an age-related increase in both proteins.
.
Serum levels of total tau (A) and phosphorylated tau (B) show significant positive correlations with patient age (Spearman r = 0.69 and 0.57, respectively; P < 0.05), indicating an age-related increase in both proteins.
Regarding the PANSS test results, we did not observe any correlation between the total and phosphorylated tau protein serum levels and the PANSS test results. However, we did find a weak correlation between age (Spearman R = 0.3, P value < 0.05) and a moderate correlation between the time of disease onset and negative symptoms of the PANSS test (Spearman R = 0.4, P value < 0.05) (Fig. 5).
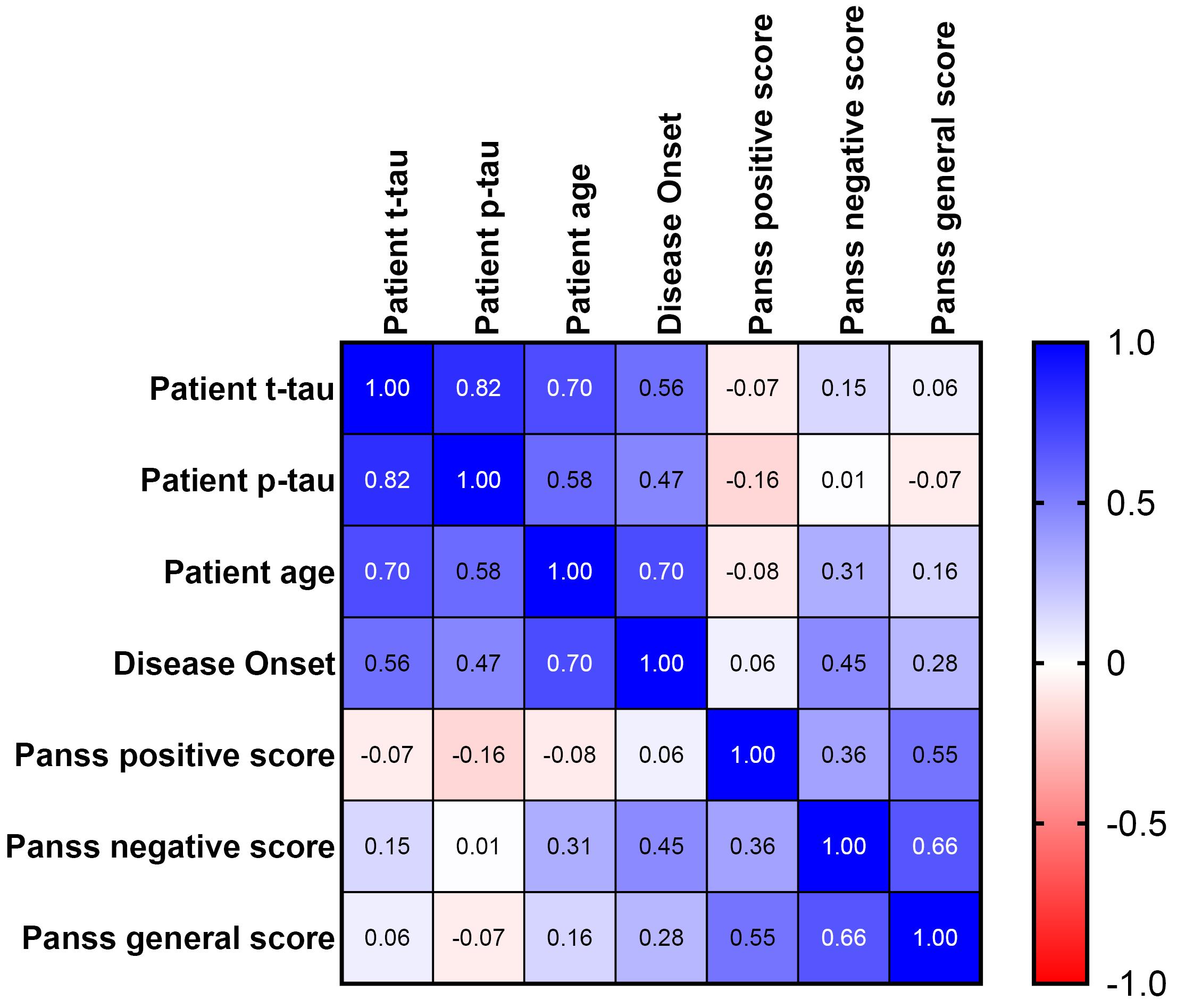
Fig. 5.
Spearman's correlation between patients’ total tau, p-tau, age, disease onset, PANSS test scores. No significant correlation was found between serum total and phosphorylated tau levels and PANSS scores. A weak positive correlation existed between age and PANSS (Spearman r = 0.3, P < 0.05), and a moderate correlation was observed between disease onset time and PANSS negative symptoms (Spearman r = 0.4, P < 0.05).
.
Spearman's correlation between patients’ total tau, p-tau, age, disease onset, PANSS test scores. No significant correlation was found between serum total and phosphorylated tau levels and PANSS scores. A weak positive correlation existed between age and PANSS (Spearman r = 0.3, P < 0.05), and a moderate correlation was observed between disease onset time and PANSS negative symptoms (Spearman r = 0.4, P < 0.05).
Furthermore, we did not find any significant correlation between the total and phosphorylated tau serum levels and the type of medication, history of ECT, or family history of the disease. Similarly, there were no significant correlations observed between the time of disease onset, number of hospitalizations, smoking, level of education, and employment (Fig. 4). To assess the correlation in the control group, we used Pearson's correlation coefficient for ordinal data and Spearman's correlation coefficient for ranking data. We found that the correlation between the total tau protein serum level and phosphorylated tau protein serum level in the control group was lower than in the patient group (Spearman R = 0.47, P value < 0.05). We also observed a moderate correlation between the age of patients and the serum level of phosphorylated tau protein (Spearman R = 0.62, P value < 0.05). Additionally, the data showed a low correlation between the age of patients and the serum level of total tau protein (Spearman R = 0.16, P value = 0.3) (Fig. 5).
To provide a comprehensive overview of the associations examined odds ratio (OR), prevalence ratio (PR), and prevalence odds ratio (POR), reported in the Tables 3 and 4 alongside the main measures.
Table 3.
Fisher's exact test for T-tau
|
Measure
|
Value
|
|
P value |
0.4391 |
| Relative risk |
1.500 |
| Odds ratio |
1.714 |
| PR |
1.5 |
| POR |
1.7 |
Table 4.
Fisher's exact test for P-tau
|
Measure
|
Value
|
|
P value |
0.1374 |
| Relative risk |
1.875 |
| Odds ratio |
2.400 |
| PR |
1.875 |
| POR |
2.4 |
Discussion
In this study, we aimed to investigate the serum levels of tau and phosphorylated tau protein in patients with schizophrenia compared to a control group. We did not find any significant differences in the serum levels of total tau protein or phosphorylated tau protein between the patient and control groups. Additionally, there was no correlation observed between these protein levels and the PANSS test results. In our study, we observed significant correlations between tau levels and age; however, the clinical implications of these associations require further investigation. The absence of correlation between tau levels and PANSS scores suggests that tau accumulation may not directly reflect the severity of schizophrenia symptoms at all disease stages. This finding highlights the possibility that other biological or environmental factors could contribute to symptom manifestation independent of tau pathology. Future research should therefore aim to clarify the clinical relevance of tau in schizophrenia, for instance by examining its role across different illness phases, its interaction with other biomarkers, and its potential contribution to disease progression rather than symptom severity alone. These findings are consistent with previous studies that have also reported no significant differences in cerebrospinal fluid levels of tau protein between patients with schizophrenia and healthy individuals. This suggests that tau protein may not be a determining factor in distinguishing between these two groups.7,8 However, it is worth noting that a study conducted in Turkey did find significant differences in serum levels of tau and phosphorylated tau protein between patients and controls, with lower levels observed in the patient group.13 This discrepancy may be due to differences in sample characteristics or other factors that require further investigation. In comparison with previous studies, our findings regarding tau levels are not entirely consistent with all reported results. Several factors may account for these discrepancies, including differences in sample characteristics such as age, disease stage, or the use of antipsychotic medication, each of which can influence neurobiological protein expression. Methodological variations, such as differences in assay techniques or data analysis approaches, may also contribute to the observed divergence. Furthermore, the potential impact of other biological factors, including comorbid conditions or genetic variations, should be considered. Addressing these variables not only helps to explain the inconsistencies across studies but also provides deeper insight into the biological mechanisms underlying tau level alterations.
Some studies have suggested a link between tau protein pathology and psychotic symptoms, but the evidence for this association is still limited.10 In patients with Alzheimer's disease and neurocognitive disorders, tau protein levels have been found to increase independence with age. However, studies in schizophrenia patients have not consistently supported the theory that cognitive decline in schizophrenia is a result of neurodegenerative disorders and tauopathy.8
One of the supporters of the neurodegenerative theory in schizophrenia performed structural and functional investigations on the brains of these patients. Supporters of the neurodegenerative hypothesis in schizophrenia have conducted structural and functional investigations on the brains of patients, which have shown changes in brain volume and structure. The decrease in the volume of the cerebral cortex and thalamus and the increase in the volume of the ventricles in these studies are considered as evidence for the existence of brain degeneration in schizophrenic patients.14 The findings of the neurodevelopmental model show that the risk factors for schizophrenia may act during the stages of synaptic reorganization and pruning that occur in early adolescence, and it is argued that the disorder in this important stage of cortical maturation is the cause of the emergence of schizophrenia and other symptoms.15 This model is supported by imaging studies reporting that the structures of the gray cortex change significantly before the onset of psychosis in individuals at high risk for schizophrenia.6-18 However, the findings of our study do not support this hypothesis, as we did not observe significant differences in tau protein levels between patients and controls. Instead, we found that the negative PANSS test scores of the patients were more correlated with age and the time of disease onset than with tau protein levels. This suggests that cognitive problems in patients with schizophrenia may not be directly related to tauopathy. It is worth noting that, in this study control participants were selected from local health care centers and universities which may introduce selection bias. Although controls were matched by age and sex, other demographic and health- related factors were not fully matched. This limitation might affect the generalizability of the findings. Therefore designing strategies to minimize selection bias in future studies are also suggested.
Conclusion
In conclusion, our study did not find significant differences in serum levels of total and phosphorylated tau protein between patients with schizophrenia and healthy controls. This suggests that tau protein may not be a determining factor in distinguishing between these two groups. However, given the nature of the research and the specific population under investigation, our study aimed to provide preliminary insights that could inform future, larger-scale investigations. Increasing the sample size would enhance the statistical power and reliability of the findings. As this study employed a cross-sectional design, causal inferences cannot be drawn and the results should be interpreted with caution. The primary objective was to examine the association between tau levels and schizophrenia symptoms at a single time point. Future longitudinal investigations are warranted to delineate the temporal dynamics and clarify potential causal relationships between tau pathology and symptom progression. Further research is needed to better understand the role of tau protein in schizophrenia and its potential association with cognitive symptoms. While our study focused on tau levels, it is important to consider other potential biomarkers and pathways that may contribute to schizophrenia pathophysiology. Neuroinflammatory markers such as IL-6 and TNF-α, alterations in dopaminergic and glutamatergic neurotransmission, oxidative stress indicators, neurotrophic factors like BDNF, and synaptic proteins including Neuregulin 1 and DISC1 represent promising avenues for future research. Investigating these biomarkers may provide a more comprehensive understanding of disease mechanisms and aid in developing targeted therapeutic strategies.
Research Highlights
What is the current knowledge?
What is new here?
-
No significant differences in serum tau levels between schizophrenia patients and healthy controls.
-
Total and phosphorylated tau are not reliable diagnostic biomarkers for schizophrenia.
-
Findings do not support tau-related neurodegeneration in schizophrenia.
Competing Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by ethics committee of Tabriz University of Medical Sciences to number IR.TBZMED.REC.1399.249 and was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all the subjects before the interview. For subjects who were under 18, written informed consent was obtained from the father or guardian of participants face to face after justifying the purpose of the study. Authors confirm that all methods were carried out in accordance with relevant guidelines and regulations.
Acknowledgements
This work was a part of the psychiatry residency dissertation of Ali Bazzaz Haghighat Talab with the Reg. No. 82488 from the department of psychiatry, Tabriz University of Medical Sciences, Tabriz, Iran. We sincerely thank research center of psychiatry and behavioral sciences.
References
- Zong X, Hu M, Li Z, Cao H, Chen X, Tang J. DNA methylation in schizophrenia: progress and challenges. Sci Bull 2015; 60:149-55. doi: 10.1007/s11434-014-0690-y [Crossref] [ Google Scholar]
- Häfner H, Maurer K, Löffler W, an der Heiden W, Munk-Jørgensen P, Hambrecht M. The ABC schizophrenia study: a preliminary overview of the results. Soc Psychiatry Psychiatr Epidemiol 1998; 33:380-6. doi: 10.1007/s001270050069 [Crossref] [ Google Scholar]
- Ballatore C, Lee VM, Trojanowski JQ. Tau-mediated neurodegeneration in Alzheimer's disease and related disorders. Nat Rev Neurosci 2007; 8:663-72. doi: 10.1038/nrn2194 [Crossref] [ Google Scholar]
- El Mammeri N, Dregni AJ, Duan P, Wang HK, Hong M. Microtubule-binding core of the tau protein. Sci Adv 2022; 8:eabo4459. doi: 10.1126/sciadv.abo4459 [Crossref] [ Google Scholar]
- Mazanetz MP, Fischer PM. Untangling tau hyperphosphorylation in drug design for neurodegenerative diseases. Nat Rev Drug Discov 2007; 6:464-79. doi: 10.1038/nrd2111 [Crossref] [ Google Scholar]
- Preuss U, Mandelkow EM. Mitotic phosphorylation of tau protein in neuronal cell lines resembles phosphorylation in Alzheimer's
disease. Eur J Cell Biol 1998; 76:176-84. doi: 10.1016/S0171-9335(98)80032-0 [Crossref] [ Google Scholar]
- Schönknecht P, Pantel J, Hartmann T, Werle E, Volkmann M, Essig M. Cerebrospinal fluid tau levels in Alzheimer's disease are elevated when compared with vascular dementia but do not correlate with measures of cerebral atrophy. Psychiatry Res 2003; 120:231-8. doi: 10.1016/s0165-1781(03)00197-5 [Crossref] [ Google Scholar]
- Frisoni GB, Prestia A, Geroldi C, Adorni A, Ghidoni R, Amicucci G. Alzheimer's CSF markers in older schizophrenia patients. Int J Geriatr Psychiatry 2011; 26:640-8. doi: 10.1002/gps.2575 [Crossref] [ Google Scholar]
- Thompson PM, Hayashi KM, de Zubicaray G, Janke AL, Rose SE, Semple J. Dynamics of gray matter loss in Alzheimer's disease. J Neurosci 2003; 23:994-1005. doi: 10.1523/jneurosci.23-03-00994.2003 [Crossref] [ Google Scholar]
- Murray PS, Kirkwood CM, Gray MC, Fish KN, Ikonomovic MD, Hamilton RL. Hyperphosphorylated tau is elevated in Alzheimer's disease with psychosis. J Alzheimers Dis 2014; 39:759-73. doi: 10.3233/jad-131166 [Crossref] [ Google Scholar]
- Wischik CM, Edwards PC, Lai RY, Gertz HN, Xuereb JH, Paykel ES. Quantitative analysis of tau protein in paired helical filament preparations: implications for the role of tau protein phosphorylation in PHF assembly in Alzheimer's disease. Neurobiol Aging 1995; 16:409-17. doi: 10.1016/0197-4580(95)97327-d [Crossref] [ Google Scholar]
- Lee D, Seo J, Jeong HC, Lee H, Lee SB. The perspectives of early diagnosis of schizophrenia through the detection of epigenomics-based biomarkers in iPSC-derived neurons. Front Mol Neurosci 2021; 14:756613. doi: 10.3389/fnmol.2021.756613 [Crossref] [ Google Scholar]
- Demirel ÖF, Cetin I, Turan Ş, Yıldız N, Sağlam T, Duran A. Total tau and phosphorylated tau protein serum levels in patients with schizophrenia compared with controls. Psychiatr Q 2017; 88:921-8. doi: 10.1007/s11126-017-9507-x [Crossref] [ Google Scholar]
- Archer T, Ricci S, Garcia D, Ricciardi MR. Neurodegenerative aspects in vulnerability to schizophrenia spectrum disorders. Neurotox Res 2014; 26:400-13. doi: 10.1007/s12640-014-9473-0 [Crossref] [ Google Scholar]
- Feinberg I. Schizophrenia: caused by a fault in programmed synaptic elimination during adolescence?. J Psychiatr Res 1982; 17:319-34. doi: 10.1016/0022-3956(82)90038-3 [Crossref] [ Google Scholar]
- Kochunov P, Hong LE. Neurodevelopmental and neurodegenerative models of schizophrenia: white matter at the center stage. Schizophr Bull 2014; 40:721-8. doi: 10.1093/schbul/sbu070 [Crossref] [ Google Scholar]
- Pantelis C, Yücel M, Wood SJ, Velakoulis D, Sun D, Berger G. Structural brain imaging evidence for multiple pathological processes at different stages of brain development in schizophrenia. Schizophr Bull 2005; 31:672-96. doi: 10.1093/schbul/sbi034 [Crossref] [ Google Scholar]
- Sun D, Phillips L, Velakoulis D, Yung A, McGorry PD, Wood SJ. Progressive brain structural changes mapped as psychosis develops in 'at risk' individuals. Schizophr Res 2009; 108:85-92. doi: 10.1016/j.schres.2008.11.026 [Crossref] [ Google Scholar]