Bioimpacts. 16:33047.
doi: 10.34172/bi.33047
Review
Emerging advancements and expanding technological scope of education and practices in pharmacy and pharmaceutical sciences
Jaleh Barar Conceptualization, Writing – original draft, Writing – review & editing, 1 
Karen Fiano Conceptualization, Writing – review & editing, 2
Matthew Seamon Conceptualization, Writing – review & editing, 2
Benedict Albensi Conceptualization, Writing – review & editing, 1
Nile Khanfar Conceptualization, Writing – review & editing, 3
Yadollah Omidi Conceptualization, Writing – original draft, Writing – review & editing, 1, *
Author information:
1Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
2Department of Pharmacy Practice, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
3Department of Sociobehavioral and Administrative Pharmacy, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
Abstract
Introduction:
The pharmacy profession stands at a pivotal moment, as emerging scientific advancements and evolving healthcare demands require adept pharmacy practitioners and scientists. The integration of precision medicine, cellular and acellular regeneration, nano and bioengineering (e.g., 3D/4D bioprinting), digital therapeutics, artificial intelligence (AI)-point-of-care testing, and treating is starting to reshape pharmacy education, practice, and patient care. Pharmacy education needs to embrace these innovations to prepare graduates for the future of practice, to optimize therapeutic outcomes, and contribute meaningfully to translational medicine.
Methods:
This review elaborates on the historical evolution toward the incoming wave of the pharmacy profession and considers the necessary educational models that might be associated with its practice.
Results:
Expanded patient care roles are essential in this new era, with clinical pharmacists increasingly working alongside physicians under collaborative practice agreements. Additionally, prescriptive authority for pharmacists is gaining traction, enhancing healthcare accessibility and medication management. The integration of digital health technologies (e.g., telepharmacy, automation, wearable medical devices, and AI-driven decision support systems) further empowers pharmacists to deliver efficient, patient-centered care. Certain prospective concentrations (e.g., precision/personalized medicine, industrial pharmacy, drug discovery and development, drug compounding and formulation, and advanced drug delivery systems and devices) can further empower pharmacy education towards healthcare needs.
Conclusion:
By embracing technological and scientific advancements, pharmacists can solidify their roles as integral healthcare providers, ensuring that the profession remains dynamic, relevant, and impactful in an evolving healthcare landscape.
Graphical Abstract
Keywords: Artificial intelligence, Automative telepharmacy, Clinical pharmacy practice expansion, Pharmacy education, Precision medicine, Pharmaceutical entrepreneurship and industry
Copyright and License Information
© 2026 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None to be declared.
Introduction
The pharmacy profession is at a crossroads. Once heralded as a pillar of healthcare, pharmacists now face shifting roles as the healthcare landscape rapidly evolves, science enters a new frontier, and artificial intelligence emerges. While medicine and science are advancing at unprecedented rates, the scope of pharmacy practice has struggled to keep pace. Counseling patients on smoking cessation or just dispensing medications is no longer of sufficient value in traditional payor systems and is being usurped by the need to advance scientific practitioners. If the pharmacy profession does not respond, it risks obsolescence. Remarkably, community pharmacy practice is evolving beyond traditional dispensing roles, and institutional pharmacy does provide value when properly situated.
Advances in science and technology have introduced new dimensions to healthcare, challenging pharmacists to redefine their roles. Vaccines, for example, have revolutionized public health by preventing infectious diseases using various types of treatments.1-9 To date, pharmacists have played an impactful critical role in vaccine deployment and administration, including COVID-19, but with today’s educational system, their involvement in the development, education, and optimization of vaccination programs seems to be underutilized.
The advancements in precision and personalized medicine demand a broader role for pharmacists beyond dispensing medications – one that integrates these innovative therapies into clinical practice and patient education. To remain relevant, pharmacies must embrace such transformation. The profession’s evolution from the compounding of herbs to managing pharmaceuticals serves as a historical precedent for its ability to adapt. However, the current pace of scientific progress necessitates a proactive approach. Pharmacists should proactively position themselves as leaders in the adoption and application of new therapies (e.g., regenerative medicine, multimodal nanomedicines and biologics, and even CRISPR-based gene editing), which can be done as part specialty. Such a training can pave the way for new opportunities. Changing demographics and urban design will transform healthcare delivery, emphasizing personalized, localized care supported by digital technologies. Advances in clinical research (e.g., preventive medicine, vaccinations, 3D printing, drone delivery, CRISPR, and implantable biosystems) will reshape the pharmaceutical landscape. Pharmacists and pharmacies must adapt to evolving roles, integrating data, artificial intelligence (AI), and technology to improve outcomes while automation handles repetitive tasks. These innovations have the potential to redefine treatment paradigms, and pharmacists are uniquely positioned to ensure their safe and effective integration into patient care. Preventive medicine is shifting from reactive treatment to proactive interventions through genomic screening, predictive analytics, and personalized risk assessment tools that identify disease susceptibility before symptoms emerge. Vaccination technologies have evolved beyond traditional platforms to include mRNA vaccines, viral vector systems, epitope-based vaccines,6 and self-amplifying mRNA vaccines,10 which can be rapidly developed and deployed against emerging pathogens using AI-assisted in-silico approaches.11 Further, 3D printing as an additive manufacturing modality is revolutionizing drug formulation by enabling on-demand production of personalized medications with customized dosages, release profiles, and combination therapies tailored to individual patient needs.12 This technology allows for complex geometric structures, such as polypills containing multiple active ingredients with distinct release kinetics, and the potential for point-of-care pharmaceutical manufacturing.13 Drone delivery systems are expanding medication access through autonomous aerial vehicles capable of transporting temperature-sensitive pharmaceuticals, emergency medications, and routine prescriptions to remote or underserved areas, reducing delivery times from hours to minutes while maintaining cold-chain integrity particularly in emergency medicine.14,15 CRISPR gene editing and related technologies (such as base editing and prime editing) are moving from research laboratories into clinical applications, offering potential cures for genetic disorders, cancer immunotherapies through CAR-T cell modification, and targeted treatments for previously incurable conditions.16,17 Implantable biosystems now encompass smart drug delivery devices, continuous glucose monitors, neurostimulators, and biosensors that provide real-time physiological monitoring and controlled medication release, creating closed-loop therapeutic systems that automatically adjust treatment based on patient response. Pharmacists and pharmacies must adapt to these evolving roles by integrating comprehensive health data from electronic health records, wearable devices, genetic testing, and patient-reported outcomes. AI and machine learning algorithms are enhancing clinical decision support through medication therapy management, drug interaction screening, adherence prediction, and optimization of pharmacotherapy regimens based on population health data and individual patient characteristics.18,19 Automation technologies (e.g., robotic dispensing systems, automated packaging, inventory management platforms, and telepharmacy infrastructure) are handling repetitive tasks, allowing pharmacists to focus on direct patient care, medication counseling, and collaborative practice agreements.20,21
Additionally, the integration of AI and digital health tools presents another frontier for pharmacy. AI can assist not only in drug discovery and development, but also in predicting patient responses to medications and in streamlining supply chain management.18,22-26 The digitalization of healthcare is transforming patient care globally, leveraging technologies like AI, blockchain, and augmented reality. These tools improve access to clinicians, real-time diagnoses, and treatments, while envisioning a cyber healthcare system integrating virtual and physical components.27 Digital health tools, such as wearable devices and mobile applications, enable real-time monitoring and personalized interventions.
Pharmacists, with their foundational understanding of pharmacology and patient care, are ideally suited to interpret data from these technologies and translate it into actionable insights for patients and healthcare providers. Advancements in digital wearable technology have significantly improved patients' ability to engage in effective self-care, offering tools for medication management, health tracking, and wellness. In this line, digital health devices and applications for self-care education might include wellness screening, insomnia, reproductive and eye disorders, home medical equipment, gastrointestinal and respiratory conditions, and pediatrics. Fully integrating digital health tools like telemedicine, electronic health records, mobile apps, and wearable devices into pharmacy education will enhance students’ ability to apply this knowledge in patient care during clinical rotations and future practice.28 Upcoming years will bring possible involvement of pharmacists in servicing patients with 3D printed pharmaceuticals and point-of-care tests.29 By embracing developing fields (e.g., precision medicine, personalized medicine, cellular and acellular therapies, bioengineering, and digital therapeutics), pharmacists can secure their relevance and become integral to modern healthcare. In this review, we aim to identify advancements in science relevant to pharmacy and briefly identify challenges and approaches toward advancement and implementation. While digital health technologies, precision medicine platforms, and advanced therapeutic modalities are rapidly transforming healthcare delivery, there remains limited systematic guidance on which emerging technologies are most relevant to pharmacy practice and how they should be integrated into pharmacy education and clinical workflows. Current pharmacy curricula and practice models have not fully adapted to prepare pharmacists for their evolving roles in interpreting data from wearable devices, managing 3D-printed pharmaceuticals, utilizing point-of-care diagnostics, and implementing digital therapeutics across diverse patient care contexts. This opinion review aims to (i) identify key scientific and technological advancements with direct relevance to pharmacy practice, including digital health tools, precision medicine, bioengineered therapies, and emerging diagnostic technologies; and (ii) discuss the challenges and practical approaches for integrating these innovations into pharmacy education and clinical practice to enhance patient care outcomes. Pharmacists possess foundational expertise in pharmacology, therapeutics, and patient care that uniquely positions them to serve as interpreters and implementers of health technology data. As digital wearables, telemedicine platforms, and personalized medicine approaches become standard components of patient self-care and clinical decision-making, pharmacists must be equipped to leverage these tools effectively. By proactively embracing emerging fields such as cellular therapies, bioengineering, and digital therapeutics, the pharmacy profession can ensure its continued relevance and establish pharmacists as integral members of technology-enabled, patient-centered healthcare teams. Preparing future pharmacists to navigate this evolving landscape is essential for optimizing medication management, improving health outcomes, and expanding the scope of pharmaceutical care in modern healthcare systems.
A glance at the historic trajectory of pharmacy
Historically, pharmacy is one of the oldest healing professions, which has always adapted to meet the demands of its time, as shown in Fig. 1. Across the ancient world, healing began as a seamless blend of belief, surgery, and drug craft. Cuneiform tablets from the Sumerian-Babylonian cities (c. 2500 BCE) already list plant resins, minerals, and animal products prescribed alongside protective incantations, showing that apothecary practice and spiritual ritual were never far apart.30 Fifteen centuries later, the Egyptian Ebers Papyrus set out 876 formulae assembled from 328 ingredients, effectively an early national pharmacopeia.31 In Achaemenid Iran, the Zoroastrian Vendīdād distilled care into the triad of “knife, herbs, and holy words,” recognising surgery, pharmacology, and counselling as complementary arms of therapy.32-34 South Asia’s Sushruta Samhitā (-c. 600 BCE) went further, codifying more than 300 operations, bespoke instruments, and postoperative herbal regimens as clear evidence that pharmacy was integral to surgery.35 On the eastern edge of the Silk Road, the Shénnóng Běnc ǎ o Jīng (1st cent. CE) rationally graded 365 medicinals by efficacy and toxicity, launching a continuously updated Chinese materia-medica tradition.36 Classical Greece marked a shift from supernatural causation to systematic observation: the Hippocratic writers insisted on clinical notes, prognosis, and treatments grounded in diet and drugs as the principles that still underpin evidence-based practice.37 Their empirical spirit culminated in Dioscorides’ five-volume De Materia Medica (c. 50–70 CE), which catalogued over a thousand simples, detailed sources, preparation methods, and dose ranges, and remained Europe’s standard pharmacological reference for more than a millennium.38 By standardizing ingredients and separating the compounding of remedies from bedside care, these texts paved the way for the professional apothecary and ensured that pharmacy would endure as a cornerstone of patient treatment in the modern era. Fig. 1 shows the evolution of pharmacy, from ancient healing traditions to professional practice.
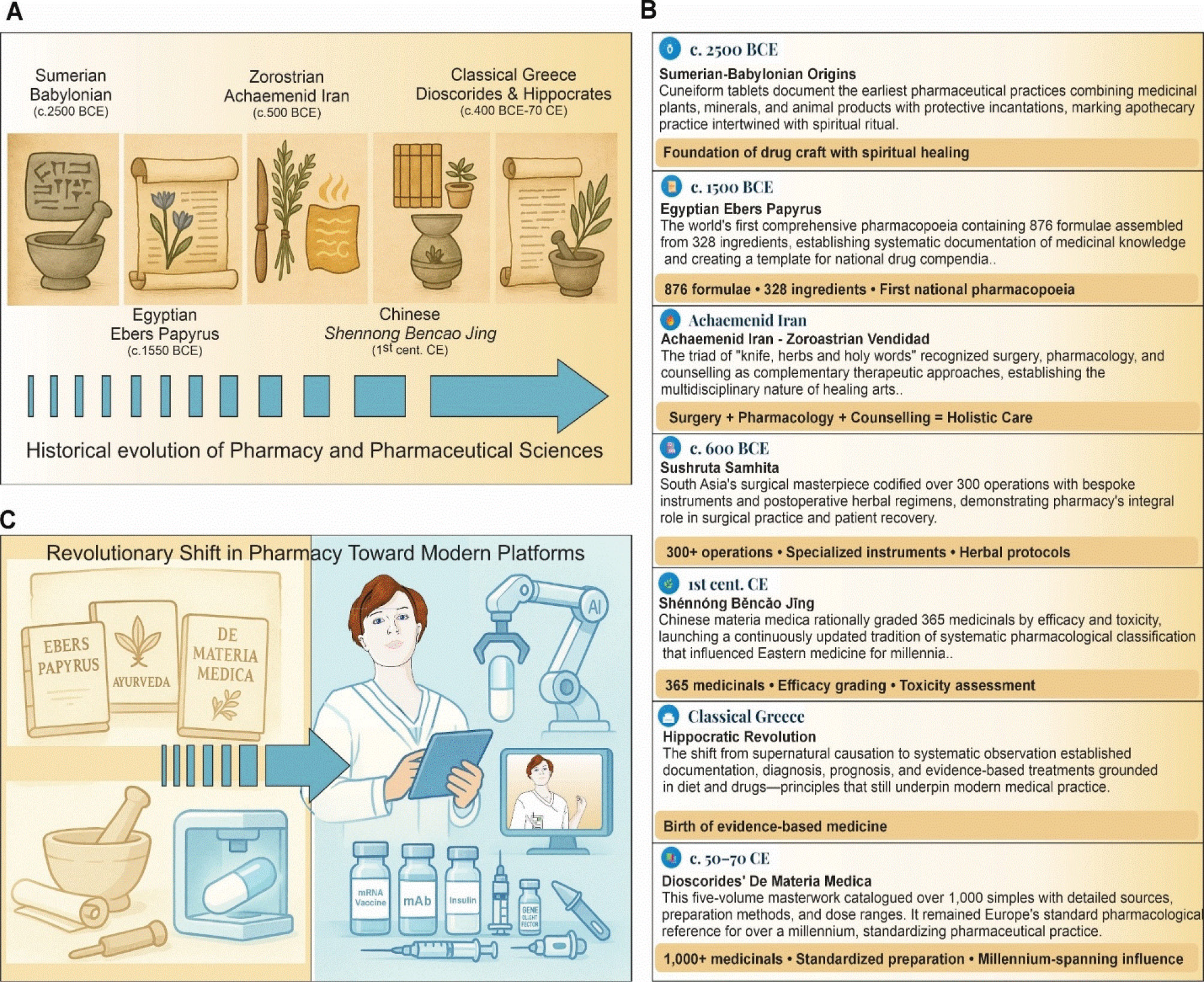
Fig. 1.
Global roots of pharmacy. (A and B) The historic timeline highlights several pivotal eras, from Sumerian-Babylonian cuneiform tablets (c. 2500 BCE) to Dioscorides’ De Materia Medica (c. 50–70 CE), which collectively shaped the evolution of pharmaceutical knowledge across Mesopotamia, Egypt, South Asia, Iran, China, and the Greco-Roman world. (C) The transition of pharmacy toward modern treatment/diagnostic medicines.
.
Global roots of pharmacy. (A and B) The historic timeline highlights several pivotal eras, from Sumerian-Babylonian cuneiform tablets (c. 2500 BCE) to Dioscorides’ De Materia Medica (c. 50–70 CE), which collectively shaped the evolution of pharmaceutical knowledge across Mesopotamia, Egypt, South Asia, Iran, China, and the Greco-Roman world. (C) The transition of pharmacy toward modern treatment/diagnostic medicines.
Today, pharmacy certainly remains a cornerstone of patient care. The classical approach to pharmacy, which is rooted in empirical observations and holistic care, provides valuable lessons for modern pharmacy educators seeking to integrate traditional wisdom with cutting-edge innovations. Today, pharmacy practice still heavily focuses on dispensing medications and providing medication counseling. These roles, while essential, represent only a fraction of what modern pharmacists can contribute.
Areas for expansion and innovation
Digital therapeutics, wearable medical devices, artificial intelligence, and machine learning
Digital therapeutics, wearable medical devices, AI, and machine learning (ML) together represent a paradigm shift in healthcare, moving from reactive care to proactive, personalized interventions. Digital therapeutics deliver evidence-based therapeutic interventions through software to prevent, manage, or treat medical disorders, often integrating real-time data from wearable devices. Wearables (e.g., smartwatches, patches, and biosensors) continuously monitor physiological parameters (e.g., heart rate, glucose levels), enabling early detection of anomalies and timely intervention.39 AI and ML algorithms serve as the analytical engine that transforms massive volumes of continuous patient data into clinically meaningful information.40-46 These computational methods include following approaches:
-
Supervised learning models that predict adverse drug events, medication non-adherence patterns, and disease progression by training on labeled historical patient data.
-
Unsupervised learning algorithms that identify previously unrecognized patient subgroups or phenotypes based on physiological patterns, enabling more precise treatment stratification.
-
Deep learning neural networks that analyze complex, multi-dimensional data streams from multiple wearable sensors simultaneously to detect subtle changes indicative of early disease states.
-
Natural language processing (NLP) that extracts relevant clinical information from patient-reported symptoms, medication histories, and electronic health records to augment automated decision support.
-
Reinforcement learning systems that continuously optimize treatment recommendations by learning from patient responses and outcomes over time.
When coupled with AI/ML algorithms, these data streams can be transformed into actionable insights through several mechanisms. Predictive analytics can forecast glycemic events in diabetic patients hours before they occur, identify patients at high risk for medication non-adherence, or detect early signs of heart failure decompensation based on weight, activity, and vital sign trends. Clinical decision support systems powered by AI can generate real-time medication dosing recommendations adjusted for individual patient pharmacokinetics, flag potential drug-drug interactions based on current physiological status, and suggest therapeutic alternatives when treatment goals are not being met. Personalized treatment algorithms analyze individual patient response patterns to optimize medication regimens, identifying optimal dosing schedules, predicting which patients will respond to specific therapies, and recommending lifestyle interventions most likely to succeed for each patient profile. Automated alert systems use ML to reduce alarm fatigue by distinguishing clinically significant deviations from normal physiological variation, prioritizing critical alerts while filtering false positives that plague traditional threshold-based monitoring. For pharmacists, AI/ML integration creates opportunities for medication therapy management at scale, where algorithms continuously analyze patient medication-taking behavior, physiological responses, and outcomes data to identify candidates for pharmacist intervention. Drug optimization platforms can suggest medication regimen simplification, identify opportunities for deprescribing, and recommend therapeutic substitutions based on real-world effectiveness data and patient-specific factors. Population health management tools enable pharmacists to identify high-risk patient cohorts, predict which patients will benefit most from targeted interventions, and allocate clinical resources efficiently based on predicted need rather than reactive crisis management.47,48 Fig. 2 shows AI-based pharmacy workflow benefits and applications, involving digital therapeutics and wearable devices for real-time patient data handling.
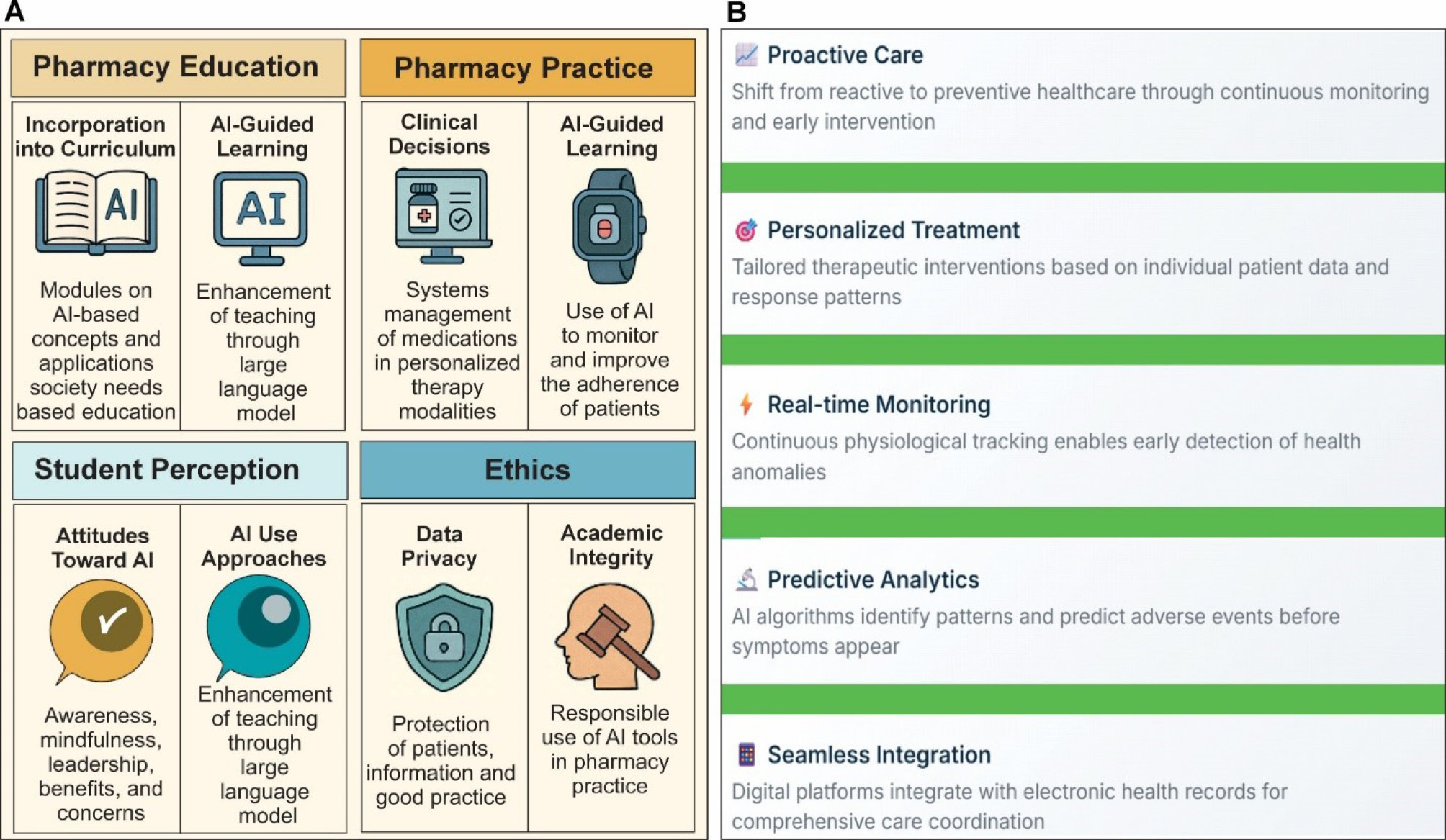
Fig. 2.
Artificial intelligence in pharmacy education and practice. (A) Infographic impacts of AI in pharmacy. The AI integrates across four domains of pharmacy, including education, practice, student perception, and ethics. The pharmacy education quadrant highlights the incorporation of AI modules into PharmD curricula, covering core concepts through AI-guided learning via large language models. In pharmacy practice, the clinical decision support systems can leverage machine learning for medication management, adverse-event prediction, and personalized dosing, as well as wearable AI technologies designed to monitor and improve patient adherence. In student perception, the infographic captures pharmacy and medical students’ awareness, attitudes, and use of AI tools, ranging from drug information retrieval to research drafting, while noting regional and disciplinary differences in uptake and confidence. In the ethics panel, AI underscores critical considerations around data privacy, cybersecurity, and academic integrity, reflecting calls for robust policies, faculty training, and ethical guidelines to govern AI adoption in both educational and clinical settings. Together, these elements provide a holistic overview of AI’s transformative potential with its challenges in shaping the future of pharmacy. (B) The key benefits and applications of AI.
.
Artificial intelligence in pharmacy education and practice. (A) Infographic impacts of AI in pharmacy. The AI integrates across four domains of pharmacy, including education, practice, student perception, and ethics. The pharmacy education quadrant highlights the incorporation of AI modules into PharmD curricula, covering core concepts through AI-guided learning via large language models. In pharmacy practice, the clinical decision support systems can leverage machine learning for medication management, adverse-event prediction, and personalized dosing, as well as wearable AI technologies designed to monitor and improve patient adherence. In student perception, the infographic captures pharmacy and medical students’ awareness, attitudes, and use of AI tools, ranging from drug information retrieval to research drafting, while noting regional and disciplinary differences in uptake and confidence. In the ethics panel, AI underscores critical considerations around data privacy, cybersecurity, and academic integrity, reflecting calls for robust policies, faculty training, and ethical guidelines to govern AI adoption in both educational and clinical settings. Together, these elements provide a holistic overview of AI’s transformative potential with its challenges in shaping the future of pharmacy. (B) The key benefits and applications of AI.
Digital therapeutics leverage algorithms to deliver tailored behavioral and pharmacological interventions. For instance, mobile applications powered by ML can adjust dosage recommendations or behavioral prompts based on patient adherence patterns and response trends.49 Such platforms have demonstrated efficacy in chronic disease management – ranging from diabetes to mental health – by offering adaptive coaching, medication reminders, and virtual cognitive-behavioral therapy sessions. Moreover, these interventions can integrate seamlessly with electronic health records, allowing healthcare providers to track patient progress remotely.18,25
Wearable medical devices serve as the cornerstone of real-time health monitoring. Advanced wearables now incorporate multiple sensors (i.e., electrocardiography, photoplethysmography, and accelerometers) to capture granular health data.39 For example, continuous glucose monitors paired with insulin pumps form closed-loop systems that autonomously maintain glycemic control. Similarly, wearable ECG patches can detect arrhythmias and alert clinicians before symptomatic events occur. The proliferation of such devices hinges on AI-driven signal processing to filter noise, detect clinically relevant patterns, and predict adverse events.49
Artificial intelligence and machine learning underpin the analytical capabilities of both digital therapeutics and wearables. Supervised learning models trained on vast datasets can identify subtle correlations between biometric signals and disease states, enhancing diagnostic accuracy.18,25,39 Unsupervised learning techniques enable the discovery of novel phenotypes by clustering patient data, which can inform the design of new therapeutic pathways.22 Deep learning architectures, such as convolutional neural networks, excel in image-based diagnostics, while natural language processing facilitates the extraction of insights from clinical notes and patient-reported outcomes.50
Integration of AI/ML in pharmacy practice further exemplifies this synergy. Algorithms aid in medication therapy management by predicting drug–drug interactions, optimizing dosing regimens, and personalizing treatment plans based on genomic and phenotypic profiles.39,49 Anthropic's Claude AI and ChatGPT-like large language models support pharmacists in drafting evidence-based recommendations and patient education materials, though ethical considerations around academic integrity and data privacy remain paramount.51 Despite tremendous promise, challenges persist. Data interoperability, cybersecurity, and regulatory hurdles must be addressed to ensure safe deployment.52 Moreover, equitable access to technology and robust validation studies are needed to avoid exacerbating healthcare disparities.53,54 As the healthcare ecosystem embraces digital therapeutics, wearables, AI, and ML, multidisciplinary collaboration among clinicians, engineers, and regulators will be essential to realize the full potential of these innovations in improving patient care.
Point-of-care testing, collaborative practice, and primary care providers
As healthcare systems shift toward preventive care, pharmacists are well-positioned to serve as primary care providers. POCT for chronic diseases, infectious conditions, where even genetic predispositions can fall under the pharmacist’s purview.55 Additionally, the emerging field of psychedelics for mental health treatment requires ethical oversight, clinical expertise, and patient education - roles that pharmacists can fulfill. Pharmacists, as some of the most accessible healthcare professionals, are uniquely positioned to bridge gaps in primary care delivery. With increasing demands on healthcare systems worldwide, including the shortage of primary care providers and the growing prevalence of chronic diseases, pharmacists have the opportunity to expand their role in clinical services. By integrating into primary care teams, offering POCT, managing chronic conditions, and prescribing medications under collaborative practice agreements, pharmacists can transform patient care while enhancing their professional relevance.
POCT allows pharmacists to offer immediate diagnostic services for conditions such as influenza, COVID-19, streptococcal pharyngitis, and hyperlipidemia. By providing these services within the community pharmacy setting, pharmacists can facilitate earlier detection and the treatment of diseases, reducing the need for costly emergency visits. For example, pharmacists can conduct hemoglobin A1c tests for diabetes management, INR monitoring for anticoagulation therapy, and even genetic screening for pharmacogenomics-based interventions. These services enhance patient engagement and improve clinical outcomes by fostering a proactive approach to health management.
Chronic disease state management
Chronic diseases represent one of the most significant challenges facing healthcare systems worldwide, with an estimated cost expected to reach $47 trillion by 2030.56 In the United States alone, 90% of the nation's $4.9 trillion in annual healthcare expenditures are attributed to chronic and mental health conditions.57 This staggering burden, combined with growing shortages of primary care providers, necessitates innovative approaches to healthcare delivery, particularly the expanded integration of pharmacists into primary care services. The transformation of pharmacy practice has been supported by collaborative practice agreements (CPAs), which allow pharmacists to work in partnership with physicians to adjust medication regimens, order laboratory tests, and implement lifestyle modifications.58,59
The evidence supporting pharmacist-led chronic disease management is substantial. Newman et al found that pharmacists can improve clinical outcomes across diabetes, hyperlipidemia, cardiovascular diseases, and respiratory conditions,60 while Greer et al concluded that pharmacist-led management achieved effects similar to usual care for resource utilization while potentially improving physiologic goal attainment.61 In diabetes management, Norton et al demonstrated that hemoglobin A1c decreased by 1.75% in collaborative pharmacist-physician care compared to only 0.16% in usual care,62 and McCarthy and Bateman reported a 2.1% reduction in A1c among patients managed by pharmacists with prescriptive authority.63 Besides, Wagner et al further showed that patients receiving pharmacist care were three to five times more likely to achieve comprehensive diabetes care quality measures.64 For hypertension, Santschi et al found significant blood pressure reductions through pharmacist interventions in a meta-analysis of over 14,000 patients,65 while Hirsch et al demonstrated superior blood pressure control with pharmacist-physician collaborative care compared to usual care.66 McCarthy and Bateman reported a 29.7 mm Hg reduction in systolic blood pressure among hypertensive patients managed by pharmacists.63 Santschi et al demonstrated that pharmacist care significantly reduced cardiovascular risk factors, including blood pressure, total cholesterol, and LDL cholesterol in diabetic patients.67
In respiratory disease management, pharmacists have shown remarkable ability to improve outcomes. Bridgeman and Wilken reported significant reductions in exacerbation rates among asthma and COPD patients following pharmacist interventions,68 while Garcia-Cardenas et al confirmed positive impacts on symptom control and prevention of exacerbations.69 Furthermore, Garcia-Cardenas et al demonstrated improved asthma control through targeted pharmacist interventions.70 The American College of Managed Care Pharmacy emphasizes that when pharmacists are recognized as providers, patient outcomes improve, satisfaction increases, and healthcare costs decrease.71 Marupuru et al found statistically significant improvements across diabetes, hypertension, and dyslipidemia through pharmacist-provided medication therapy management.72 Rahayu et al confirmed that pharmacists in interprofessional teams facilitate access to primary care and improve patient outcomes.73 Rodis et al demonstrated that 52.84% of patients with uncontrolled diabetes achieved target A1c levels following pharmacist interventions in community health centers.74
The movement toward formal provider status recognition represents the natural progression of this evidence base. Cernasev et al discuss the evolution from collaborative practice agreements toward comprehensive provider status, which would enable reimbursement for pharmacist services and ensure sustainability across diverse settings.75 Given that approximately 90% of Americans reside within two miles of a community pharmacy, expanded pharmacist authority could significantly improve access to primary care, particularly in underserved communities. The integration of pharmacists into primary care represents a paradigm shift with the potential to significantly enhance healthcare delivery. The extensive evidence demonstrates that pharmacists can independently manage chronic conditions, achieving outcomes comparable to or better than traditional models. Through CPAs, pharmacists optimize medication therapy, provide continuous education, and address adherence barriers in ways that complement overburdened primary care systems. As healthcare systems grapple with escalating chronic disease burden, constrained resources, and workforce shortages. Therefore, the full integration of pharmacists as recognized providers offers a practical, evidence-based solution to address critical gaps in care access and quality while reducing overall healthcare costs.
Mental health and psychedelic therapies
Mental health is an area where pharmacists’ expertise is underutilized.76 With the growing acceptance of psychedelic therapies for treatment-resistant depression, post-traumatic stress disorder (PTSD), anxiety, and autism, pharmacists can play a critical role in this emerging field.77 Their responsibilities could include dosing and monitoring of psychedelic compounds such as psilocybin, ketamine, and 3,4-methylenedioxymethamphetamine (MDMA), ensuring patient safety and therapeutic efficacy. Of these, for example, MDMA (commonly known as ecstasy or molly) is a psychoactive drug that affects mood and perception, primarily by increasing the activity of three neurotransmitters (i.e., serotonin, dopamine, and norepinephrine) in the brain, resulting in heightened feelings of euphoria, emotional closeness, increased energy, and sensory enhancement. Additionally, pharmacists can provide medication therapy management for patients with complex psychiatric conditions such as PTSD, addressing potential interactions and side effects.78
Precision medicine and personalized therapy
Generally, classical medicine remains the backbone for broad public-health impact and cost-effective care. Personalized medicine emphasizes holistic, patient-centered adjustments within existing clinical frameworks. Precision medicine layers cutting-edge molecular and digital data on top of personalization, narrowing treatment to biologically defined subsets for maximum efficacy and minimal harm. Furthermore, the emergence of digital therapeutics and personalized medicine signals a shift in the healthcare paradigm. Digital therapeutics utilize technology to treat, manage, and prevent diseases through software-driven interventions, often in combination with traditional medications. Personalized medicine is medical treatment that tailors treatment strategies based on individual genetic, environmental, and lifestyle factors, offering unprecedented opportunities for precision care.79,80 Table 1 provides a side-by-side comparison of classical, personalized, and precision medicine.
Table 1.
A side-by-side comparison of classical, personalized, and precision medicine
|
Dimension
|
Classical (one-size-fits-all) medicine
|
Personalized medicine
|
Precision medicine
|
| Primary goal |
Identify treatments that work for the average patient with a given diagnosis. |
Tailor therapy to an individual’s clinical features, lifestyle, and preferences. |
Stratify patients into molecularly defined sub-groups and match them to targeted interventions. |
| Key data inputs |
• Symptoms & signs
• Basic labs & imaging
• Population-level RCT evidence |
Classical data plus:
• Detailed family & social history
• Comorbidities
• Patient-reported outcomes |
Personalized data plus:
• Genomics / epigenomics
• Transcriptomics / proteomics / metabolomics
• Digital biomarkers, real-time wearables
• AI-driven pattern recognition |
| Typical treatment approach |
Standard guideline-based drug or procedure for everyone meeting diagnostic criteria. |
Adjust dose, drug choice, rehab plan, counseling style, etc., for a single patient. |
Use biomarkers (e.g., EGFR, BRCA), companion diagnostics, or multi-omic signatures to select or design an intervention for a subset of patients. |
| Population scale |
Entire disease population. |
Individual patient. |
Molecularly homogeneous cohorts (often 1–10 % of the total population). |
| Examples |
• First-line amoxicillin for community pneumonia
• Thiazide diuretic for essential hypertension |
• Switching antidepressants based on side-effect profile
• Custom physiotherapy schedule for an athlete |
• Trastuzumab only for HER2-positive breast cancer
• mRNA therapy for a specific CFTR mutation
• CAR-T cells designed for a patient’s tumor antigens |
| Advantages |
• Simple logistics
• Lower upfront cost
• Large evidence base |
• Holistic care improves adherence & satisfaction• Considers lifestyle and preferences |
• Higher efficacy and fewer adverse effects in the targeted group
• Enables drug repurposing and basket trials
• Drives biomarker discovery |
| Limitations |
• Variable efficacy
• Unnecessary toxicity for non-responders |
• Relies on clinician judgment; may still miss molecular drivers |
• Expensive diagnostics
• Small trial populations complicate evidence generation
• Equity concerns (omics data bias) |
| Regulatory & reimbursement landscape |
Well-defined, generic pathways. |
Similar to classical, a few distinct regulations. |
Requires co-approval of test + therapy; value-based or outcomes-based pricing emerging. |
| Ethical considerations |
Fair access, but possible overtreatment. |
Risk of clinician bias if “personalization” is subjective. |
Data privacy (genomics, wearables), unequal access to testing, and possible genetic discrimination. |
| Future trajectory |
Still vital for many common conditions. |
Merging with precision through better data capture, such as electronic health records, and wearable systems. |
Moving toward “pan-omics” & AI-guided preventive precision health; potential for CRISPR, digital twins. |
For more details, readers are directed to read the following citations.81-86
Notably, precision medicine has gained prominence as an innovative healthcare approach tailored to individual genetic profiles, lifestyle factors, and environmental contexts.87 Within this movement, pharmacists hold a pivotal position due to their direct involvement in medication management and patient care. As a result, pharmacy education programs are increasingly focused on equipping future practitioners with the requisite competencies in pharmacogenomics and related fields.88 Despite these, yet, several challenges remain, including the need for instructional strategies that go beyond traditional lectures to foster higher-order thinking and practical application.89 Fig. 3 shows the pharmacists' impactful interplay in terms of precision medicine and advanced therapies in collaboration with health care professionals.
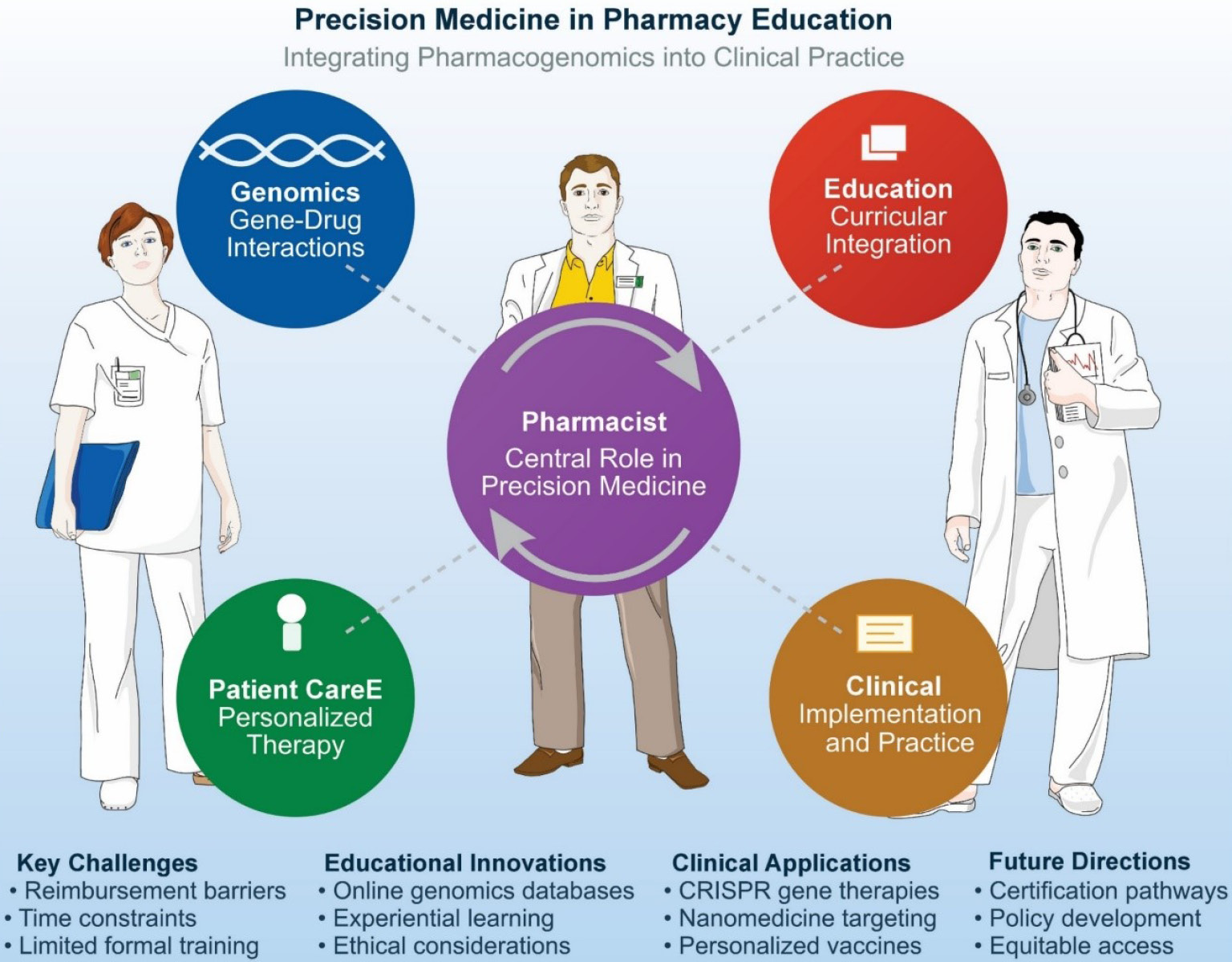
Fig. 3.
Interplay of pharmacists in precision medicine in collaboration with physicians, nurses, and other health care professionals.
.
Interplay of pharmacists in precision medicine in collaboration with physicians, nurses, and other health care professionals.
One key aspect is ensuring that pharmacists appreciate the social and ethical dimensions accompanying precision medicine. Introducing students to these issues early in their education helps them to develop more nuanced diagnostic and therapeutic strategies for diverse patient populations. On the practical front, pharmacy educators must consider creative and interactive teaching resources. For instance, online cancer genomics databases can facilitate experiential learning and bridge theory with real-world oncologic applications.90 By engaging with actual clinical data, students gain a clearer understanding of how genetic variations influence treatment decisions and patient outcomes. This approach complements didactic content by illustrating the dynamic application of pharmacogenomics in oncology.
Evidence suggests that prior exposure to precision medicine concepts during pharmacy school positively affects pharmacists’ willingness to implement these strategies in practice.87 Community pharmacists, in particular, may benefit from structured training programs covering genetic testing methodologies, data interpretation, and ethical considerations, ultimately enhancing their capacity to offer personalized patient care. Such training, when combined with the appropriate curricular reforms, can produce graduates well-prepared to navigate the rapidly evolving landscape of precision medicine.
Pharmacists, as accessible healthcare providers, play a pivotal role in identifying gene–drug interactions, educating patients, and collaborating with prescribers to optimize therapy. However, studies indicate that many pharmacists still feel underprepared to implement personalized services and require further education.86,91 Despite demonstrated enthusiasm, pharmacists report barriers to widespread personalized medicine adoption, including reimbursement issues, time constraints, and limited formal training. Addressing these challenges involves collaborative efforts among academic institutions, industry, and policymakers to develop standardized certification pathways, robust evidence bases, and user-friendly PGx resources.92 Moreover, educators must underscore ethical considerations, such as data privacy and equitable access, ensuring that personalized care remains patient-centric and inclusive. Ultimately, strengthening pharmacy education in precision medicine paves the way for more efficient, safe, and patient-tailored interventions. Altogether, pharmacists can play a pivotal role in implementing pharmacogenomic/ pharmacoproteomic testing, interpreting results, and optimizing drug therapy. For example, in cancer treatment, pharmacists could guide the use of CRISPR-based gene therapies or nanomedicine to target specific mutations. The profession may also address advanced therapies such as hormone replacement for genetic disorders and personalized vaccines that are designed using a patient’s unique genetic profile.
Cell therapies and regenerative medicine
As pharmacists expand their roles from dispensing medications to providing patient-centered care, incorporating regenerative therapies into practice is another leading area open to growth and education. This includes the growing complexity of regenerative interventions, including advanced cell therapies, tissue engineering, and stem cell-based products, all of which demand a deep understanding of both clinical efficacy and regulatory requirements.93 Regenerative medicine aims to repair or replace damaged tissues and organs by harnessing the body’s intrinsic healing mechanisms and utilizing engineered constructs. From diabetic polyneuropathy treatments employing dental pulp stem cells,94 and wound healing95 to novel fibrin-targeting delivery systems for cardiac repair,96 the breadth of potential therapies highlights the need for robust educational frameworks. Pharmacy students, as future healthcare professionals, must be versed in drug development pathways, immunological considerations, and patient safety standards to ensure the responsible adoption of regenerative products.97 As evidenced by the growing interest in mesenchymal stem cells and exosomes, pharmacists will increasingly engage in developing formulations that optimize cell viability and targeted drug delivery. Ultimately, pharmacy education serves as a cornerstone for equipping practitioners to evaluate evidence, guide informed decision-making, and combat misinformation surrounding regenerative approaches. By offering specialized training and fostering research collaborations, pharmacy programs can support the safe, ethical, and effective integration of regenerative medicine into routine clinical practice. Further, cellular therapies (e.g., stem cell treatments, CAR-T cell therapy, dendritic cell (DC) vaccines, and regenerative medicine approaches) are revolutionizing the treatment modalities of diseases at the molecular and cellular levels. For instance, CAR-T cell therapy, which involves engineering a patient’s own immune cells to target and destroy cancer cells, has shown remarkable success in treating certain types of leukemia and lymphoma. Likewise, the therapeutic impacts of DC vaccines against different malignancies are undisputable. Pharmacists can play a critical role in the preparation, storage, and administration of these complex therapies, ensuring their safety and efficacy.
Despite their potential, cellular and acellular therapies present several challenges that must be addressed. These include high costs, complex manufacturing processes, and stringent storage and handling requirements. Pharmacists must acquire specialized knowledge in these areas to effectively manage these therapies. This includes understanding the principles of bioprocessing, cold chain logistics, and the regulatory frameworks governing advanced therapy medicinal products. Fig. 4 illustrates the pharmacists' roles in regenerative medicine and advanced therapies.
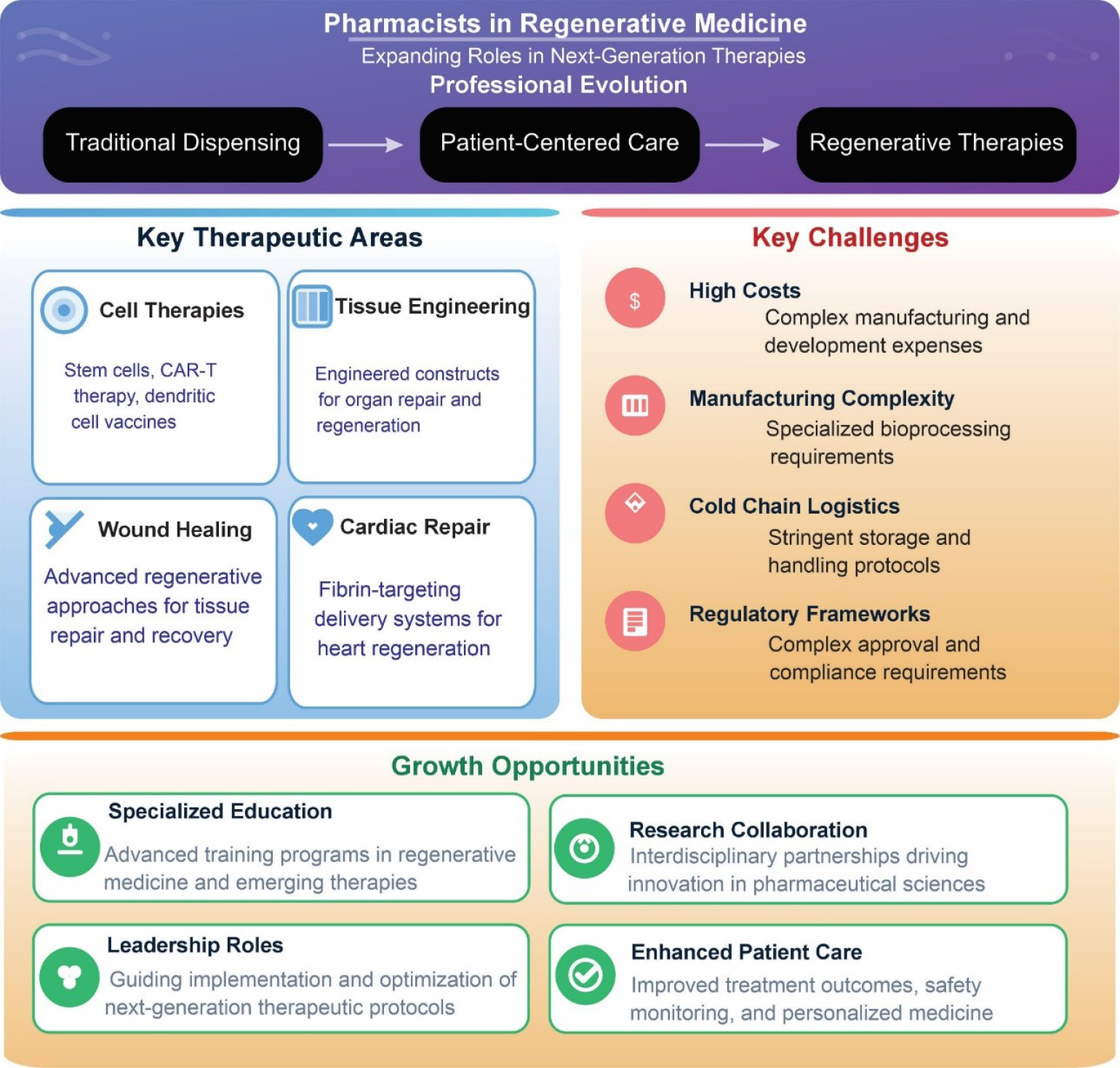
Fig. 4.
Pharmacists’ roles in regenerative medicine and advanced therapies. The future of pharmacy practice is going to be largely shaped by emerging technologies, most likely by embracing regenerative medicine and autonomous activity in the personalization of pharmacotherapy. Pharmacists position themselves as leaders in the next generation of health care delivery. This transformation requires continuous learning, interdisciplinary collaboration, and expanded practice roles to ensure safe, ethical, and effective integration of advanced therapies.
.
Pharmacists’ roles in regenerative medicine and advanced therapies. The future of pharmacy practice is going to be largely shaped by emerging technologies, most likely by embracing regenerative medicine and autonomous activity in the personalization of pharmacotherapy. Pharmacists position themselves as leaders in the next generation of health care delivery. This transformation requires continuous learning, interdisciplinary collaboration, and expanded practice roles to ensure safe, ethical, and effective integration of advanced therapies.
By embracing these advancements, pharmacists can position themselves as leaders in the delivery of next-generation therapies, ultimately enhancing patient care and outcomes. Altogether, cellular and acellular therapies represent a transformative opportunity for the pharmacy profession. By expanding their expertise and embracing these innovative treatments, pharmacists can play a pivotal role in shaping the future of healthcare. This requires a commitment to continuous learning, interdisciplinary collaboration, and advocacy for expanded practice roles.
Acellular therapies
Acellular therapies involve the use of biological products such as extracellular vesicles, exosomes, and protein-based treatments. These therapies are gaining traction for their ability to modulate biological processes and deliver targeted interventions without the risks associated with living cells. The use of acellular bioengineered scaffolds, made from various bionanomaterials, provides a framework for cell growth and tissue regeneration. Pharmacists can contribute to the development and distribution of these scaffolds, ensuring their biocompatibility and effectiveness in regenerative applications. Acellular therapy represents a rapidly emerging area in regenerative medicine that holds significant implications for pharmacy education. Recent developments in acellular therapies, including extracellular vesicle-based treatments, highlight the shift from cell transplantation to harnessing the therapeutic properties of cellular secretomes.98,99 These changes underscore the importance of equipping future pharmacists with an interdisciplinary skill set that spans pharmaceutical sciences, regulatory affairs, and clinical applications. Current pharmacy curricula often emphasize chemical pharmacology and compounding, but must evolve to incorporate foundational knowledge of bioengineering and regenerative biology. Acellular biomaterials, such as scaffolds or extracellular vesicles, offer less complex pathways for regulatory approval compared to cell-based treatments, presenting unique challenges and opportunities for pharmacists. As therapies targeting cartilage regeneration, bone healing, and tissue repair increasingly rely on biomolecules rather than entire cells, pharmacists’ expertise in product handling, stability, storage, and patient counseling will be crucial.100,101 Moreover, a comprehensive understanding of the pathophysiology of conditions like osteoarthritis, where acellular strategies can mitigate inflammatory pathways, enables pharmacists to collaborate effectively with orthopedic teams.102 Notably, incorporating laboratory-based learning experiences and clinical case studies into pharmacy education can help bridge the gap between conventional pharmacotherapy and emerging regenerative modalities.
Parallel to the rise of 3D printing, acellular therapy is attracting considerable interest in pharmaceutical research. Unlike cell-based therapies, acellular approaches focus on delivering bioactive molecules and scaffolds without relying on living cells. In regenerative medicine, for instance, acellular scaffolds can facilitate tissue repair and targeted treatment strategies. As these therapies gain prominence, pharmacists will need a thorough grounding in formulation science, biocompatible materials, and the regulatory frameworks that oversee advanced manufacturing technologies.103 By merging 3D printing and acellular therapy into pharmacy education, institutions can better prepare graduates to handle emerging challenges. This preparation extends beyond conventional clinical settings, as research indicates potential applications for on-demand manufacturing in extreme or remote environments, such as space missions.104,105 During extended voyages, the ability to create personalized therapies, including acellular treatments, could significantly enhance healthcare outcomes and reduce logistical burdens.
Bioengineering and bioprinting
Bioengineering and bioprinting are transformative fields that intersect with pharmacy practice, offering groundbreaking solutions for conditions previously deemed incurable. Bioprinting tissue regeneration involves creating functional tissue to repair or replace damaged organs and tissues, while bioengineering applies engineering principles to biological systems to develop therapeutic solutions. Together, these fields are reshaping the landscape of modern medicine and present unique opportunities for pharmacists to expand their roles. Pharmacy education is experiencing a rapid transformation, driven by technological progress and the increasing demand for personalized healthcare.106 One key area of innovation is three-dimensional (3D) printing, which has opened new avenues for producing individualized dosage forms and sophisticated drug delivery systems. Pharmacy curricula are thus evolving to incorporate instruction on 3D printing techniques (e.g., selective laser sintering, binder deposition, and inkjet printing), which allow precise control over dose, release profiles, and design complexity.103,107
Moreover, integrating these technologies within pharmacy programs promotes interdisciplinary collaboration, equipping future professionals with the skills to communicate effectively with engineers, clinicians, and biomedical scientists. As the field continues to evolve, a holistic approach that emphasizes both the technical and patient-focused aspects of acellular therapy and 3D printing will be essential. Bioprinting involves the layer-by-layer deposition of bio-inks containing living cells and biomaterials to construct tissues or organ structures. For example, researchers have successfully bioprinted skin grafts for burn patients and are exploring the development of bioprinted organs for transplantation. Pharmacists can play a pivotal role in ensuring the compatibility, safety, and efficacy of bio-inks and other bioproducts used in these procedures. By doing so, pharmacy education will remain at the forefront of innovation, preparing graduates to contribute meaningfully to patient care and to the broader development of personalized medicine.
Pharmacists are also essential in the emerging field of microfluidics-based technologies, such as cell/tissue/organ-on-a-chip technology. Such micro-/nano-engineered systems mimic the architecture and function of human organs, providing a platform for drug testing and disease modeling. By collaborating with bioengineers, pharmacists can contribute to the development of personalized medicine approaches, optimizing drug therapies based on patient-specific organ models. Another critical aspect of tissue regeneration is the use of stem cells and growth factors to stimulate the body’s natural healing processes.
Cutting-edge examples of bioengineering include the development of organ-on-a-chip platforms, which mimic the microarchitecture and functions of human organs. These systems are being used for drug testing, disease modeling, and personalized medicine applications. Pharmacists, with their expertise in drug formulation and pharmacodynamics, can collaborate with bioengineers to optimize therapies tested on these platforms. As mentioned earlier, another frontier in tissue regeneration is the use of decellularized matrices. These are scaffolds derived from donor tissues or synthetic materials, which have had all cells removed, leaving behind only the extracellular matrix. These scaffolds can be seeded with a patient’s own cells to promote tissue regeneration, reducing the risk of immune rejection. For instance, decellularized heart valves and blood vessels have been used in cardiovascular surgeries, and research is underway to develop decellularized liver and kidney scaffolds for organ repair. Pharmacists can contribute by ensuring the biocompatibility and safety of these scaffolds, as well as by managing their storage and preparation for clinical use.
Advancements in bioengineering are also exploring the potential of smart biomaterials that respond to environmental stimuli, such as temperature, pH, or specific enzymes, to release drugs or facilitate tissue regeneration. These materials could enable highly targeted and controlled therapies, minimizing side effects and enhancing treatment outcomes. Pharmacists, as drug delivery experts, are well-positioned to oversee the formulation and application of these biomaterials in clinical settings.
3D Bioprinting
Pharmacy programs should be increasingly incorporating 3D printing modules into their coursework to provide hands-on experience with personalized drug formulations and medical devices.108 Traditional manufacturing techniques, such as tableting and encapsulation, often limit students’ exposure to newer technologies. By contrast, 3D printing offers unparalleled customization, enabling learners to design, prototype, and test drug-loaded constructs.109 This experiential learning fosters critical thinking and problem-solving skills, as students must consider polymer selection, extrusion temperature, and post-printing quality control parameters.110
Moreover, the introduction of such technologies aligns with the broader push toward patient-centric care. When pharmacy students interact with 3D printers, they understand how personalized dosage forms can improve therapeutic outcomes, particularly for populations requiring flexible dosing, such as pediatric or geriatric patients.111 In this context, the skill set extends beyond conventional pharmaceutics to include digital modeling, software usage, and familiarity with regulatory perspectives.
Notably, a bridging theory and practice must be addressed, by which 3D printing in pharmacy education can help illustrate theoretical concepts, such as polymer science, drug stability, and controlled release mechanisms.112 Students can translate these concepts into tangible prototypes.113 For instance, in designing a 3D-printed dosage form, learners might adjust the infill percentage of a tablet to modulate dissolution rates—a concept closely tied to polymer matrix design.114 Such hands-on projects clarify how solid-state chemistry and manufacturing parameters jointly influence drug release kinetics.
From an educational standpoint, this technology underscores the shift toward patient-focused outcomes. By developing polypills in the laboratory, students recognize how 3D printing can reduce pill burden, potentially enhance adherence, and lead to better therapeutic results.115 This understanding is especially pertinent for complex conditions, such as cancer or neurological disorders, where polypharmacy is common.
Lessons in 3D printing processes help students develop skills in selecting optimal printing methods for specific therapeutic applications, such as microneedles for transdermal delivery or orodispersible films (ODFs), also known as oral fast-dissolving films. ODFs can be used for patients when the fast release is necessary or for those with swallowing difficulties.
Despite the promise of these technologies, significant challenges remain. Bioprinting faces hurdles in scaling up production for clinical use, ensuring vascularization of printed tissues, and adhering to strict regulatory requirements. Similarly, organ-on-a-chip platforms and decellularized matrices require rigorous validation to ensure their reliability and reproducibility in diverse patient populations.
Moreover, the high costs associated with these innovations limit their accessibility. Pharmacists can play a critical role in advocating for policies that make these therapies more affordable and widely available. They can also help develop cost-effective methods for manufacturing and distributing bioengineered products, bridging the gap between innovation and patient care through translational research and development.
To harness the full potential of bioengineering and tissue regeneration, pharmacy education and practice must evolve. Training programs should include courses on biomaterials science, tissue engineering, and advanced drug delivery systems. Collaborative efforts between pharmacy schools, bioengineering departments, and biotechnology companies can accelerate the translation of these technologies into practice.
In clinical settings, pharmacists can act as intermediaries among engineers, clinicians, and patients, ensuring that bioengineered therapies are safe, effective, and accessible. They can also participate in research to optimize the delivery and integration of these therapies, contributing to the advancement of precision medicine. Fig. 5 shows a schematic illustration of the applications of bioengineering technologies.
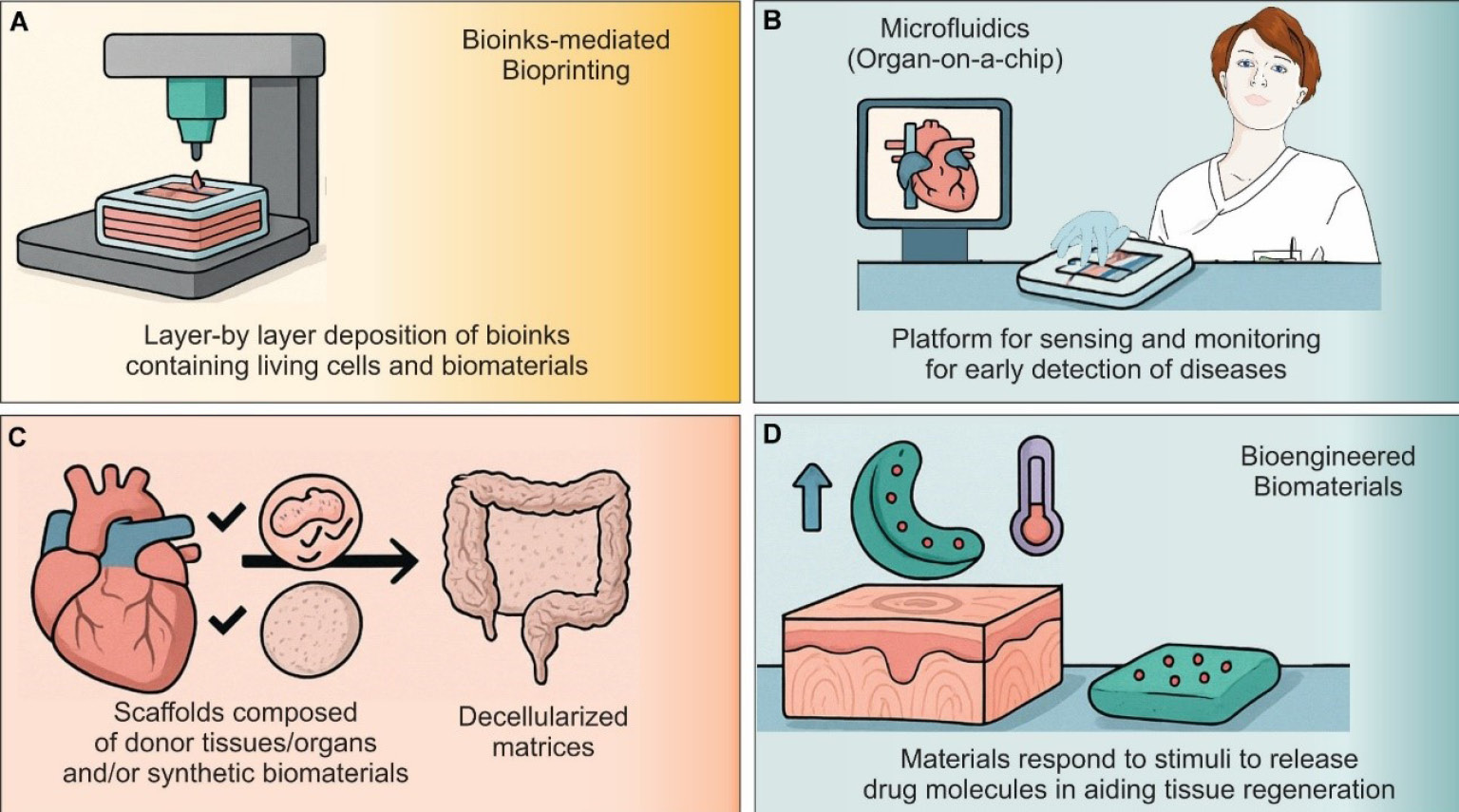
Fig. 5.
Core bioengineering and bioprinting technologies in pharmacy practice. A detailed educational schematic presenting four foundational technologies at the interface of pharmacy and bioengineering. (A) A schematic infographic illustrating the integration of 3D bioprinting as a layer-by-layer deposition of bio-inks containing living cells and biomaterials for tissue constructs. (B) Microfluidic Organ-on-a-Chip technology, which is a miniaturized perfused systems that recapitulate organ microarchitecture for drug testing and disease modeling. (C) Decellularized matrices that are extracellular scaffolds derived from donor tissues or synthetic materials, repopulated with patient cells to promote tissue regeneration. (D) Smart biomaterials as the engineered constructs that respond to environmental stimuli (e.g., pH, temperature, enzymes) to achieve controlled drug release and enhance healing.
.
Core bioengineering and bioprinting technologies in pharmacy practice. A detailed educational schematic presenting four foundational technologies at the interface of pharmacy and bioengineering. (A) A schematic infographic illustrating the integration of 3D bioprinting as a layer-by-layer deposition of bio-inks containing living cells and biomaterials for tissue constructs. (B) Microfluidic Organ-on-a-Chip technology, which is a miniaturized perfused systems that recapitulate organ microarchitecture for drug testing and disease modeling. (C) Decellularized matrices that are extracellular scaffolds derived from donor tissues or synthetic materials, repopulated with patient cells to promote tissue regeneration. (D) Smart biomaterials as the engineered constructs that respond to environmental stimuli (e.g., pH, temperature, enzymes) to achieve controlled drug release and enhance healing.
Notably, the integration of modules into pharmacy curricula is an inevitable emerging event, which seems to be associated with many challenges and opportunities. As an example, starting from coursework (“3D Bioprinting”), students progress to hands-on operation of a 3D printer producing personalized drug formulations. Key steps include polymer selection, fabrication of drug-loaded constructs, and manipulation of infill percentage to modulate release kinetics. Representative end-products (e.g., microneedle arrays for transdermal delivery and orodispersible polypills) demonstrate the technology’s potential to tailor therapy for diverse patient populations.
Concluding remarks and vision for the future
The transformation of pharmacy education and practice requires cultural and technological shifts within the profession itself, which need to be advocated through some new legislation. These include an expanded scope of practice, also involving personalized medicine and bioengineering, and methods to adopt AI into practice. This perhaps demands cooperation among different domains of science and technologies. Historically, pharmacists have been seen as compounders and then dispensers of medications, but this perception must change as science flourishes. Pharmacists must advocate for their expanded role as integral members of the healthcare team, capable of bridging the gap between medical advancements and patient outcomes. This advocacy involves engaging in policy discussions, pursuing advanced training, and embracing interdisciplinary collaboration. As an example, from futuristic prospects, “pan-omics”, which refers to the integrated analysis of multiple “omes” (complete sets of molecular data) within a biological system, can meet the need of capturing the full complexity of health and disease. Rather than studying one class of biomolecule in isolation (e.g., genomic, transcriptomic, epigenomic, proteomic, or metabolomic data), pan-omics seeks to layer and interrelate data from all these domains. As a result, the features of pan-omics can include (i) multi-layered data integration, (ii) systems-level insight, (iii) network and pathway modeling that can identify cross-talk between pathways, and uncover novel therapeutic targets, and (iv) personalized, preventive health. Its applications seem to be vast, covering (i) digital twins by creating in silico replicas of individual patients by integrating their pan-omic data to simulate disease trajectories or drug responses, (ii) CRISPR-guided therapies through pan-omic data, (iii) biomarker discovery. The future of pharmacy lies in integration—integrating cutting-edge science, personalized care, and ethical oversight into a unified practice. By awakening to these possibilities, pharmacists can redefine their profession as an indispensable pillar of modern healthcare, ensuring not just survival but lasting impact and leadership, and continue their critical role in the healthcare team, which should create a new model as a public enterprise in the healthcare system.
Review Highlights
What is the current knowledge?
-
The pharmacy profession is at a pivotal moment requiring practitioners to adapt to emerging scientific advancements and evolving healthcare demands.
-
Clinical pharmacists increasingly work alongside physicians under collaborative practice agreements to provide expanded patient care.
-
Pharmacy education must prepare graduates for future practice to optimize therapeutic outcomes and contribute to translational medicine.
-
Pharmacists need to solidify their role as integral healthcare providers to ensure the profession remains dynamic and relevant.
What is new here?
-
Precision medicine, cellular/acellular regeneration, nano and bioengineering (e.g., 3D/4D bioprinting), and AI-driven point-of-care testing are beginning to reshape pharmacy practice and education.
-
Prescriptive authority for pharmacists is gaining traction, enhancing healthcare accessibility and medication management capabilities.
-
Digital health technologies such as telepharmacy, automation, wearable medical devices, and AI-driven decision support systems are empowering pharmacists to deliver efficient, patient-centered care.
-
Prospective educational concentrations in precision/personalized medicine, industrial pharmacy, drug discovery and development, compounding, and advanced drug delivery systems are emerging to address future healthcare needs.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
Not applicable.
Declaration of AI-assisted Tools in the Writing Procedure
The authors declare that Claude AI (Anthropic) was used, in accordance with applicable licensing terms, to improve the clarity and readability of the manuscript.
Acknowledgements
The Authors would like to acknowledge the Nova Southeastern University support.
References
- Barzegari A, Saeedi N, Zarredar H, Barar J, Omidi Y. The search for a promising cell factory system for production of edible vaccine. Hum Vaccin Immunother 2014; 10:2497-502. doi: 10.4161/hv.29032 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Saeedi N, Barzegari A, Dehghani J, Omidi Y. Current status and future prospective of vaccine development against Echinococcus granulosus. Biologicals 2018; 51:1-11. doi: 10.1016/j.biologicals.2017.10.003 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Naghili B, Saeedi N, Parvizpour S, Nematollahi A. A novel in silico minigene vaccine based on CD4(+) T-helper and B-cell epitopes of EG95 isolates for vaccination against cystic echinococcosis. Comput Biol Chem 2018; 72:150-63. doi: 10.1016/j.compbiolchem.2017.11.008 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Daghighkia H, Nematollahi A, Omidi Y. A novel B- and helper T-cell epitopes-based prophylactic vaccine against Echinococcus granulosus. Bioimpacts 2018; 8:39-52. doi: 10.15171/bi.2018.06 [Crossref] [ Google Scholar]
- Parvizpour S, Razmara J, Pourseif MM, Omidi Y. In silico design of a triple-negative breast cancer vaccine by targeting cancer testis antigens. Bioimpacts 2019; 9:45-56. doi: 10.15171/bi.2019.06 [Crossref] [ Google Scholar]
- Parvizpour S, Pourseif MM, Razmara J, Rafi MA, Omidi Y. Epitope-based vaccine design: a comprehensive overview of bioinformatics approaches. Drug Discov Today 2020; 25:1034-42. doi: 10.1016/j.drudis.2020.03.006 [Crossref] [ Google Scholar]
- Pourseif MM, Parvizpour S, Jafari B, Dehghani J, Naghili B, Omidi Y. A domain-based vaccine construct against SARS-CoV-2, the causative agent of COVID-19 pandemic: development of self-amplifying mRNA and peptide vaccines. Bioimpacts 2021; 11:65-84. doi: 10.34172/bi.2021.11 [Crossref] [ Google Scholar]
- Safary A, Akbarzadeh-Khiavi M, Barar J, Omidi Y. SARS-CoV-2 vaccine-triggered autoimmunity: Molecular mimicry and/or bystander activation of the immune system. Bioimpacts 2023; 13:269-73. doi: 10.34172/bi.2023.27494 [Crossref] [ Google Scholar]
- Omidi Y, Pourseif MM, Ansari RA, Barar J. Design and development of mRNA and self-amplifying mRNA vaccine nanoformulations. Nanomedicine (Lond) 2024; 19:2699-725. doi: 10.1080/17435889.2024.2419815 [Crossref] [ Google Scholar]
- Pourseif MM, Masoudi-Sobhanzadeh Y, Azari E, Parvizpour S, Barar J, Ansari R. Self-amplifying mRNA vaccines: Mode of action, design, development and optimization. Drug Discov Today 2022; 27:103341. doi: 10.1016/j.drudis.2022.103341 [Crossref] [ Google Scholar]
- Salemi A, Pourseif MM, Omidi Y. Next-generation vaccines and the impacts of state-of-the-art in-silico technologies. Biologicals 2021; 69:83-5. doi: 10.1016/j.biologicals.2020.10.002 [Crossref] [ Google Scholar]
- Singh R, Wani AK, Peter L, Randlova K, Hruska J, Chopra C. The Role of 3D Printing in Revolutionizing Pharmaceuticals and Medicine. Mini Rev Med Chem 2025; 25:1539-54. doi: 10.2174/0113895575381660250930170819 [Crossref] [ Google Scholar]
- Mandal B, Rathi S, Singh S. 3D Printing in Pharmaceuticals: A Mini Review of Materials, Techniques and Challenges. Zhongguo Ying Yong Sheng Li Xue Za Zhi 2025; 41:e20250029. doi: 10.62958/j.cjap.2025.028 [Crossref] [ Google Scholar]
- Johnson AM, Cunningham CJ, Arnold E, Rosamond WD, Zègre-Hemsey JK. Impact of Using Drones in Emergency Medicine: What Does the Future Hold?. Open Access Emerg Med 2021; 13:487-98. doi: 10.2147/oaem.S247020 [Crossref] [ Google Scholar]
- Granholm F, Tin D, Ciottone GR. Not war, not terrorism, the impact of hybrid warfare on emergency medicine. Am J Emerg Med 2022; 62:96-100. doi: 10.1016/j.ajem.2022.10.021 [Crossref] [ Google Scholar]
- Iyer SP, Sica RA, Ho PJ, Prica A, Zain J, Foss FM. Safety and activity of CTX130, a CD70-targeted allogeneic CRISPR-Cas9-engineered CAR T-cell therapy, in patients with relapsed or refractory T-cell malignancies (COBALT-LYM): a single-arm, open-label, phase 1, dose-escalation study. Lancet Oncol 2025; 26:110-22. doi: 10.1016/s1470-2045(24)00508-4 [Crossref] [ Google Scholar]
- Huang G, Tang Y, Zhang S, Ning H, Xu J, Li F. Multifunctional nano-polymer-based targeted delivery system for CRISPR/Cas9-Mediated hepatocellular carcinoma therapy. Int J Pharm 2026; 687:126392. doi: 10.1016/j.ijpharm.2025.126392 [Crossref] [ Google Scholar]
- Smoke S. The two dimensions of pharmacy artificial intelligence tools. Am J Health Syst Pharm 2025; 82:e113-e6. doi: 10.1093/ajhp/zxae293 [Crossref] [ Google Scholar]
- Maqbool T, Ishaq H, Shakeel S, Zaib Un Nisa A, Rehman H, Kashif S. Future pharmacy practitioners’ insights towards integration of artificial intelligence in healthcare education: Preliminary findings from Karachi, Pakistan. PLoS One 2025; 20:e0314045. doi: 10.1371/journal.pone.0314045 [Crossref] [ Google Scholar]
- Maleki M, Mardani A, Kakemam E, Huertas-Zurriaga A, Vaismoradi M. Robot-assisted medication management in home care and long-term care settings: a mixed-method systematic review. Expert Rev Pharmacoecon Outcomes Res 2025; 25:1167-82. doi: 10.1080/14737167.2025.2537190 [Crossref] [ Google Scholar]
- Abimanyu EPB, Satibi Satibi, Endarti D. Digital Technologies in Hospital Pharmacy: A Systematic Review of Their Impact on Efficiency, Safety, and Inventory Management. J Prev Med Public Health 2026; 59:1-11. doi: 10.3961/jpmph.25.495 [Crossref] [ Google Scholar]
- Cain J, Malcom DR, Aungst TD. The Role of Artificial Intelligence in the Future of Pharmacy Education. Am J Pharm Educ 2023; 87:100135. doi: 10.1016/j.ajpe.2023.100135 [Crossref] [ Google Scholar]
- Nelson SD. Artificial intelligence and the future of pharmacy. Am J Health Syst Pharm 2024; 81:83-4. doi: 10.1093/ajhp/zxad316 [Crossref] [ Google Scholar]
- Batson C, Mara D. The Pharmacy Students’ Guide to Artificial Intelligence-AI. J Pediatr Pharmacol Ther 2024; 29:85-9. doi: 10.5863/1551-6776-29.1.85 [Crossref] [ Google Scholar]
- Smoke S. Artificial intelligence in pharmacy: A guide for clinicians. Am J Health Syst Pharm 2024; 81:641-6. doi: 10.1093/ajhp/zxae051 [Crossref] [ Google Scholar]
- González-Pérez Y, Montero Delgado A, Martinez Sesmero JM. Approaching artificial intelligence to Hospital Pharmacy. Farm Hosp 2024; 48 Suppl 1:S35-s44. doi: 10.1016/j.farma.2024.02.007 [Crossref] [ Google Scholar]
- Trenfield SJ, Awad A, McCoubrey LE, Elbadawi M, Goyanes A, Gaisford S. Advancing pharmacy and healthcare with virtual digital technologies. Adv Drug Deliv Rev 2022; 182:114098. doi: 10.1016/j.addr.2021.114098 [Crossref] [ Google Scholar]
- Wong JC, Hekimyan L, Cruz FA, Brower T. Identifying Pertinent Digital Health Topics to Incorporate into Self-Care Pharmacy Education. Pharmacy (Basel) 2024; 12:96. doi: 10.3390/pharmacy12030096 [Crossref] [ Google Scholar]
- Barar J, Seamon M, Omidi Y. The emergence of advanced technologies in the pharmacy profession and the need for education: The case of point-of-care sensing systems and 3D printing of pharmaceuticals. Bioimpacts 2026; 16:31081. doi: 10.34172/bi.31081 [Crossref] [ Google Scholar]
- Mark JJ. Medicine in Ancient Mesopotamia. World History Encyclopedia; 2023.
- Metwaly AM, Ghoneim MM, Eissa IH, Elsehemy IA, Mostafa AE, Hegazy MM. Traditional ancient Egyptian medicine: A review. Saudi J Biol Sci 2021; 28:5823-32. doi: 10.1016/j.sjbs.2021.06.044 [Crossref] [ Google Scholar]
- Moghadasi AN. History of Multiple Sclerosis in Iran. Arch Iran Med 2020; 23:211-5. [ Google Scholar]
- Darmesteter J. The Vendidad. In: Müller Max, editor. The Zend-Avesta: Oxford: Clarendon Press; 1880.
- Nayernouri T. A Brief History of Ancient Iranian Medicine. Arch Iran Med 2015; 18:549-51. [ Google Scholar]
- Dave T, Habte A, Vora V, Sheikh MQ, Sanker V, Gopal SV. Sushruta: The Father of Indian Surgical History. Plast Reconstr Surg Glob Open 2024; 12:e5715. doi: 10.1097/gox.0000000000005715 [Crossref] [ Google Scholar]
- Zhao Z, Guo P, Brand E. A concise classification of bencao (materia medica). Chin Med 2018; 13:18. doi: 10.1186/s13020-018-0176-y [Crossref] [ Google Scholar]
- Kleisiaris CF, Sfakianakis C, Papathanasiou IV. Health care practices in ancient Greece: The Hippocratic ideal. J Med Ethics Hist Med 2014; 7:6. [ Google Scholar]
- Osbaldeston TA, Wood RPA. Dioscorides’ De Materia Medica: A New Indexed Version in Modern English. Johannesburg: Ibidis Press; 2000.
- Chalasani SH, Syed J, Ramesh M, Patil V, Pramod Kumar TM. Artificial intelligence in the field of pharmacy practice: A literature review. Explor Res Clin Soc Pharm 2023; 12:100346. doi: 10.1016/j.rcsop.2023.100346 [Crossref] [ Google Scholar]
- Safdari R, Ferdousi R, Aziziheris K, Niakan-Kalhori SR, Omidi Y. Computerized techniques pave the way for drug-drug interaction prediction and interpretation. Bioimpacts 2016; 6:71-8. doi: 10.15171/bi.2016.10 [Crossref] [ Google Scholar]
- Masoudi-Sobhanzadeh Y, Omidi Y, Amanlou M, Masoudi-Nejad A. DrugR+: A comprehensive relational database for drug repurposing, combination therapy, and replacement therapy. Comput Biol Med 2019; 109:254-62. doi: 10.1016/j.compbiomed.2019.05.006 [Crossref] [ Google Scholar]
- Masoudi-Sobhanzadeh Y, Omidi Y, Amanlou M, Masoudi-Nejad A. Trader as a new optimization algorithm predicts drug-target interactions efficiently. Sci Rep 2019; 9:9348. doi: 10.1038/s41598-019-45814-8 [Crossref] [ Google Scholar]
- Masoudi-Sobhanzadeh Y, Motieghader H, Omidi Y, Masoudi-Nejad A. A machine learning method based on the genetic and world competitive contests algorithms for selecting genes or features in biological applications. Sci Rep 2021; 11:3349. doi: 10.1038/s41598-021-82796-y [Crossref] [ Google Scholar]
- Torkamannia A, Omidi Y, Ferdousi R. A review of machine learning approaches for drug synergy prediction in cancer. Brief Bioinform 2022; 23:bbac075. doi: 10.1093/bib/bbac075 [Crossref] [ Google Scholar]
- Daneshvar NH, Masoudi-Sobhanzadeh Y, Omidi Y. A voting-based machine learning approach for classifying biological and clinical datasets. BMC Bioinformatics 2023; 24:140. doi: 10.1186/s12859-023-05274-4 [Crossref] [ Google Scholar]
- Torkamannia A, Omidi Y, Ferdousi R. SYNDEEP: a deep learning approach for the prediction of cancer drugs synergy. Sci Rep 2023; 13:6184. doi: 10.1038/s41598-023-33271-3 [Crossref] [ Google Scholar]
- Simpson MD, Qasim HS. Clinical and Operational Applications of Artificial Intelligence and Machine Learning in Pharmacy: A Narrative Review of Real-World Applications. Pharmacy (Basel) 2025; 13:41. doi: 10.3390/pharmacy13020041 [Crossref] [ Google Scholar]
- Mahajan A, Heydari K, Powell D. Wearable AI to enhance patient safety and clinical decision-making. NPJ Digit Med 2025; 8:176. doi: 10.1038/s41746-025-01554-w [Crossref] [ Google Scholar]
-
Roosan D, Padua P, Khan R, Khan H, Verzosa C, Wu Y. Effectiveness of ChatGPT in clinical pharmacy and the role of artificial intelligence in medication therapy management. J Am Pharm Assoc (2003) 2024; 64: 422–8.e8. doi: 10.1016/j.japh.2023.11.023.
- Gimeno-Ballester V, Trigo-Vicente C. [Translated article] The role of artificial intelligence in scientific publishing: perspectives from hospital pharmacy. Farm Hosp 2024; 48:T246-t51. doi: 10.1016/j.farma.2024.07.009 [Crossref] [ Google Scholar]
- Mortlock R, Lucas C. Generative artificial intelligence (Gen-AI) in pharmacy education: Utilization and implications for academic integrity: A scoping review. Explor Res Clin Soc Pharm 2024; 15:100481. doi: 10.1016/j.rcsop.2024.100481 [Crossref] [ Google Scholar]
-
Marín CMH, Boquet EM, Andrés JLP. Ciberseguridad, una prioridad de los servicios de farmacia en la era de la inteligencia artificial. Farmacia hospitalaria 2024. 48: 195–7. doi: 10.1016/j.farma.2024.08.001.
- Hasan HE, Jaber D, Al Tabbah S, Lawand N, Habib HA, Farahat NM. Knowledge, attitude and practice among pharmacy students and faculty members towards artificial intelligence in pharmacy practice: A multinational cross-sectional study. PLoS One 2024; 19:e0296884. doi: 10.1371/journal.pone.0296884 [Crossref] [ Google Scholar]
-
Hasan HE, Jaber D, Khabour OF, Alzoubi KH. Perspectives of Pharmacy Students on Ethical Issues Related to Artificial Intelligence: A Comprehensive Survey Study. Res Sq 2024; rs.3.rs-4302115. doi: 10.21203/rs.3.rs-4302115/v1.
- Kehrer JP, James DE. The Role of Pharmacists and Pharmacy Education in Point-of-Care Testing. Am J Pharm Educ 2016; 80:129. doi: 10.5688/ajpe808129 [Crossref] [ Google Scholar]
- Hacker K. The Burden of Chronic Disease. Mayo Clinic Proceedings: Innovations, Quality & Outcomes 2024; 8:112-9. doi: 10.1016/j.mayocpiqo.2023.08.005 [Crossref] [ Google Scholar]
- Centers for Disease C, Prevention. Fast Facts: Health and Economic Costs of Chronic Conditions 2025.
- Centers for Disease C, Prevention. Collaborative Practice Agreements and Pharmacists’ Patient Care Services: A Resource for Pharmacists 2013.
- Sachdev G, Kliethermes MA, Vernon V, Leal S, Crabtree G. Current status of prescriptive authority by pharmacists in the United States. J Am Coll Clin Pharm 2020; 3:807-17. doi: 10.1002/jac5.1245 [Crossref] [ Google Scholar]
- Newman TV, San-Juan-Rodriguez A, Parekh N, Swart ECS, Klein-Fedyshin M, Shrank WH. Impact of community pharmacist-led interventions in chronic disease management on clinical, utilization, and economic outcomes: An umbrella review. Res Social Adm Pharm 2020; 16:1155-65. doi: 10.1016/j.sapharm.2019.12.016 [Crossref] [ Google Scholar]
- Greer N, Bolduc J, Geurkink E, Rector T, Olson K. Pharmacist-Led Chronic Disease Management: A Systematic Review of Effectiveness and Harms Compared to Usual Care. Washington (DC): Department of Veterans Affairs (US); 2016.
- Norton MC, Haftman ME, Buzzard LN. Impact of physician-pharmacist collaboration on diabetes outcomes and health care use. J Am Board Fam Med 2020; 33:745-53. doi: 10.3122/jabfm.2020.05.200044 [Crossref] [ Google Scholar]
- McCarthy C, Thomas Bateman M. Impact of pharmacist‐led chronic disease management in a Federally Qualified Health Center. J Am Coll Clin Pharm 2022; 5:1263-77. doi: 10.1002/jac5.1720 [Crossref] [ Google Scholar]
- Wagner TD, Dixon DL, Shin Y, Dozmorov M, Musselman KT, Buffington TM. Impact of pharmacist-physician collaborative care on hemoglobin A1c and blood pressure quality measure achievement in primary care. J Manag Care Spec Pharm 2025; 31:565-77. doi: 10.18553/jmcp.2025.31.6.565 [Crossref] [ Google Scholar]
- Santschi V, Chiolero A, Colosimo AL, Platt RW, Taffé P, Burnier M. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. J Am Heart Assoc 2014; 3:e000718. doi: 10.1161/jaha.113.000718 [Crossref] [ Google Scholar]
- Hirsch JD, Steers N, Adler DS, Kuo GM, Morello CM, Lang M. Primary care-based, pharmacist-physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther 2014; 36:1244-54. doi: 10.1016/j.clinthera.2014.06.030 [Crossref] [ Google Scholar]
- Santschi V, Chiolero A, Paradis G, Colosimo AL, Burnand B. Pharmacist interventions to improve cardiovascular disease risk factors in diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2012; 35:2706-17. doi: 10.2337/dc12-0369 [Crossref] [ Google Scholar]
- Bridgeman MB, Wilken LA. Essential Role of Pharmacists in Asthma Care and Management. J Pharm Pract 2021; 34:149-62. doi: 10.1177/0897190020927274 [Crossref] [ Google Scholar]
- Garcia-Cardenas V, Armour C, Benrimoj SI, Martinez-Martinez F, Rotta I, Fernandez-Llimos F. Pharmacists' interventions on clinical asthma outcomes: a systematic review. Eur Respir J 2016; 47:1134-43. doi: 10.1183/13993003.01497-2015 [Crossref] [ Google Scholar]
- García-Cárdenas V, Sabater-Hernández D, Kenny P, Martínez-Martínez F, Faus MJ, Benrimoj SI. Effect of a pharmacist intervention on asthma control A cluster randomised trial. Respir Med 2013; 107:1346-55. doi: 10.1016/j.rmed.2013.05.014 [Crossref] [ Google Scholar]
- Academy of Managed Care Pharmacy. Provider Status for Pharmacists; 2023. https://www.amcp.org/legislative-regulatory-position/provider-status-pharmacists.
- Marupuru S, Roether A, Guimond AJ, Stanley C, Pesqueira T, Axon DR. A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia. Healthcare (Basel) 2022; 10:1207. doi: 10.3390/healthcare10071207 [Crossref] [ Google Scholar]
- Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. J Multidiscip Healthc 2021; 14:1701-10. doi: 10.2147/JMDH.S309938 [Crossref] [ Google Scholar]
- Rodis JL, Sevin A, Awad MH, Porter B, Glasgow K, Hornbeck Fox C. Improving Chronic Disease Outcomes Through Medication Therapy Management in Federally Qualified Health Centers. J Prim Care Community Health 2017; 8:324-31. doi: 10.1177/2150131917701797 [Crossref] [ Google Scholar]
- Cernasev A, Aruru M, Clark S, Patel K, DiPietro Mager N, Subramaniam V. Empowering public health pharmacy practice-moving from collaborative practice agreements to provider status in the US. Pharmacy (Basel) 2021; 9:57. doi: 10.3390/pharmacy9010057 [Crossref] [ Google Scholar]
- Romney M, Robinson RF, Boyle J. Mental Health Pharmacists: Increasing Necessary Mental Health Service Delivery. Fed Pract 2022; 39:106-8. doi: 10.12788/fp.0237 [Crossref] [ Google Scholar]
- Bartecki J. From Stigma to Breakthrough: Psychedelic Medicin. Pharm Times. 2025; 19(2): Available from: https://www.pharmacytimes.com/view/from-stigma-to-breakthrough-psychedelic-medicine.
- Hippensteele A. Navigating the Psychedelic Renaissance: Emerging Mental Health Therapies and the Pharmacist’s Role. Pharm Times. 2024. Available from: https://www.pharmacytimes.com/view/navigating-the-psychedelic-renaissance-emerging-mental-health-therapies-and-the-pharmacist-s-role.
- Anonymous Anonymous. AMCP Partnership Forum: Digital Therapeutics-What Are They and Where Do They Fit in Pharmacy and Medical Benefits?. J Manag Care Spec Pharm 2020; 26:674-81. doi: 10.18553/jmcp.2020.19418 [Crossref] [ Google Scholar]
- Bulaj G, Coleman M, Johansen B, Kraft S, Lam W, Phillips K. Redesigning Pharmacy to Improve Public Health Outcomes: Expanding Retail Spaces for Digital Therapeutics to Replace Consumer Products That Increase Mortality and Morbidity Risks. Pharmacy (Basel) 2024; 12:107. doi: 10.3390/pharmacy12040107 [Crossref] [ Google Scholar]
- Sarhangi N, Nikfar S, Hasanzad M, Larijani B. Precision medicine path at personalized medicine research center/endocrinology and metabolism research institute: A systematic review. J Diabetes Metab Disord 2024; 23:1507-13. doi: 10.1007/s40200-020-00708-9 [Crossref] [ Google Scholar]
- Al-Maini M, Maindarkar M, Kitas GD, Khanna NN, Misra DP, Johri AM. Artificial intelligence-based preventive, personalized and precision medicine for cardiovascular disease/stroke risk assessment in rheumatoid arthritis patients: a narrative review. Rheumatol Int 2023; 43:1965-82. doi: 10.1007/s00296-023-05415-1 [Crossref] [ Google Scholar]
- Marques L, Costa B, Pereira M, Silva A, Santos J, Saldanha L. Advancing Precision Medicine: A Review of Innovative In Silico Approaches for Drug Development, Clinical Pharmacology and Personalized Healthcare. Pharmaceutics 2024; 16:332. doi: 10.3390/pharmaceutics16030332 [Crossref] [ Google Scholar]
- Zeng S, Qing Q, Xu W, Yu S, Zheng M, Tan H. Personalized anesthesia and precision medicine: a comprehensive review of genetic factors, artificial intelligence, and patient-specific factors. Front Med (Lausanne) 2024; 11:1365524. doi: 10.3389/fmed.2024.1365524 [Crossref] [ Google Scholar]
-
Aththanagoda A, Kulathilake K, Abdullah NA. Precision and Personalization: How Large Language Models Redefining Diagnostic Accuracy in Personalized Medicine - A Systematic Literature Review. IEEE J Biomed Health Inform 2025; Pp. doi: 10.1109/jbhi.2025.3584179.
- Alexander KM, Divine HS, Hanna CR, Gokun Y, Freeman PR. Implementation of personalized medicine services in community pharmacies: perceptions of independent community pharmacists. J Am Pharm Assoc (2003) 2014; 54:510-7, 5 p following 7. doi: 10.1331/JAPhA.2014.13041 [Crossref] [ Google Scholar]
- Naimat F, Fahrni ML, Purushothaman S, Abdul Ghani MN, Chumnumwat S, Babar ZU. Community pharmacists’ perceived value on precision medicine, desired training components, and exposure during pharmacy education: Malaysia’s experience. Front Pharmacol 2022; 13:978141. doi: 10.3389/fphar.2022.978141 [Crossref] [ Google Scholar]
- Rao US, Mayhew SL, Rao PS. Strategies for implementation of an effective pharmacogenomics program in pharmacy education. Pharmacogenomics 2015; 16:905-11. doi: 10.2217/pgs.15.50 [Crossref] [ Google Scholar]
- Kisor DF, Calinski DM, Farrell CL. Beyond the didactic lecture: pharmacogenomics in pharmacy education. Per Med 2018; 15:9-12. doi: 10.2217/pme-2017-0056 [Crossref] [ Google Scholar]
- Pasupuleti D, Nguyen T, Nahta R. Using Online Cancer Genomics Databases to Provide Teaching Resources for Pharmacy Education. Am J Pharm Educ 2022; 86:ajpe8683. doi: 10.5688/ajpe8683 [Crossref] [ Google Scholar]
- Siamoglou S, Koromina M, Moy FM, Mitropoulou C, Patrinos GP, Vasileiou K. What Do Students in Pharmacy and Medicine Think About Pharmacogenomics and Personalized Medicine Education? Awareness, Attitudes, and Perceptions in Malaysian Health Sciences. Omics 2021; 25:52-9. doi: 10.1089/omi.2020.0178 [Crossref] [ Google Scholar]
- Radhakrishnan A, Kuppusamy G. Theoretical Formulation Strategies towards Neutralizing Inter-individual Variability Associated with Tacrolimus Immunosuppressant Therapy: A Case Study on Nextgeneration Personalized Medicine. Curr Drug Metab 2021; 22:939-56. doi: 10.2174/1389200222666211015153317 [Crossref] [ Google Scholar]
- Beheshtizadeh N, Gharibshahian M, Pazhouhnia Z, Rostami M, Zangi AR, Maleki R. Commercialization and regulation of regenerative medicine products: Promises, advances and challenges. Biomed Pharmacother 2022; 153:113431. doi: 10.1016/j.biopha.2022.113431 [Crossref] [ Google Scholar]
- Samiei M, Dalir Abdollahinia E, Amiryaghoubi N, Fathi M, Barar J, Omidi Y. Injectable thermosensitive chitosan/gelatin hydrogel for dental pulp stem cells proliferation and differentiation. Bioimpacts 2023; 13:63-72. doi: 10.34172/bi.2022.23904 [Crossref] [ Google Scholar]
- Humenik F, Danko J, Krešáková L, Vdoviaková K, Vrabec V, Vasilová E. A Chitosan-Based Biomaterial Combined with Mesenchymal Stem Cell-Conditioned Medium for Wound Healing and Skin Regeneration. Int J Mol Sci 2023; 24:16080. doi: 10.3390/ijms242216080 [Crossref] [ Google Scholar]
- Huang Z, Song Y, Pang Z, Li M, Guliya Y, Shen Y. Fibrin-targeting delivery: a novel platform for cardiac regenerative medicine. J Cell Mol Med 2016; 20:2410-3. doi: 10.1111/jcmm.12912 [Crossref] [ Google Scholar]
- Sankova MV, Beeraka NM, Oganesyan MV, Rizaeva NA, Sankov AV, Shelestova OS. Recent developments in Achilles tendon risk-analyzing rupture factors for enhanced injury prevention and clinical guidance: Current implications of regenerative medicine. J Orthop Translat 2024; 49:289-307. doi: 10.1016/j.jot.2024.08.024 [Crossref] [ Google Scholar]
- Burdick JA, Mauck RL, Gorman JH, 3rd 3rd, Gorman RC. Acellular biomaterials: an evolving alternative to cell-based therapies. Sci Transl Med 2013; 5:176ps4. doi: 10.1126/scitranslmed.3003997 [Crossref] [ Google Scholar]
- Jarrige M, Frank E, Herardot E, Martineau S, Darle A, Benabides M. The Future of Regenerative Medicine: Cell Therapy Using Pluripotent Stem Cells and Acellular Therapies Based on Extracellular Vesicles. Cells 2021; 10:240. doi: 10.3390/cells10020240 [Crossref] [ Google Scholar]
- Altomare D, Di Matteo B, Kon E. Conservative Treatment for Ankle Cartilage: Cellular and Acellular Therapies: A Systematic Review. Foot Ankle Clin 2024; 29:253-63. doi: 10.1016/j.fcl.2023.07.003 [Crossref] [ Google Scholar]
- Brown MG, Brady DJ, Healy KM, Henry KA, Ogunsola AS, Ma X. Stem Cells and Acellular Preparations in Bone Regeneration/Fracture Healing: Current Therapies and Future Directions. Cells 2024; 13:1045. doi: 10.3390/cells13121045 [Crossref] [ Google Scholar]
- Jammes M, Contentin R, Cassé F, Galéra P. Equine osteoarthritis: Strategies to enhance mesenchymal stromal cell-based acellular therapies. Front Vet Sci 2023; 10:1115774. doi: 10.3389/fvets.2023.1115774 [Crossref] [ Google Scholar]
- Carou-Senra P, Rodríguez-Pombo L, Awad A, Basit AW, Alvarez-Lorenzo C, Goyanes A. Inkjet Printing of Pharmaceuticals. Adv Mater 2024; 36:e2309164. doi: 10.1002/adma.202309164 [Crossref] [ Google Scholar]
- Katakam P, Bhavaraju MLR, Narayana TV, Bhandari K, Sriram N, Sisinty VS. Navigating the Challenges of 3D Printing Personalized Medicine in Space Explorations: A Comprehensive Review. Crit Rev Ther Drug Carrier Syst 2024; 41:89-110. doi: 10.1615/CritRevTherDrugCarrierSyst.2024051126 [Crossref] [ Google Scholar]
- Tocci D, Ducai T, Stoute CAB, Hopkins G, Sabbir MG, Beheshti A. “Monitoring inflammatory, immune system mediators, and mitochondrial changes related to brain metabolism during space flight”. Front Immunol 2024; 15:1422864. doi: 10.3389/fimmu.2024.1422864 [Crossref] [ Google Scholar]
- Lepowsky E, Tasoglu S. 3D printing for drug manufacturing: A perspective on the future of pharmaceuticals. Int J Bioprint 2018; 4:119. doi: 10.18063/IJB.v4i1.119 [Crossref] [ Google Scholar]
-
Mathew E, Pitzanti G, Larrañeta E, Lamprou DA. 3D Printing of Pharmaceuticals and Drug Delivery Devices. Pharmaceutics [serial on the Internet] 2020; 12. doi: 10.3390/pharmaceutics12030266.
- Singhvi G, Patil S, Girdhar V, Chellappan DK, Gupta G, Dua K. 3D-printing: an emerging and a revolutionary technology in pharmaceuticals. Panminerva Med 2018; 60:170-3. doi: 10.23736/s0031-0808.18.03467-5 [Crossref] [ Google Scholar]
- Chahuan A, Verma A, Shekho D, Mishra R, Awasthi A. Revolutionizing the World of Pharmaceuticals: Unleashing the Game-Changing Power of 3D Printing. Curr Drug Targets 2024; 25:513-6. doi: 10.2174/0113894501304163240429081741 [Crossref] [ Google Scholar]
- Azad MA, Olawuni D, Kimbell G, Badruddoza AZM, Hossain MS, Sultana T. Polymers for Extrusion-Based 3D Printing of Pharmaceuticals: A Holistic Materials-Process Perspective. Pharmaceutics 2020; 12:124. doi: 10.3390/pharmaceutics12020124 [Crossref] [ Google Scholar]
- Khalaf AT, Wei Y, Wan J, Zhu J, Peng Y, Abdul Kadir SY. Bone Tissue Engineering through 3D Bioprinting of Bioceramic Scaffolds: A Review and Update. Life (Basel) 2022; 12:903. doi: 10.3390/life12060903 [Crossref] [ Google Scholar]
- Wadher K, Trivedi R, Wankhede N, Kale M, Umekar M. 3D printing in pharmaceuticals: An emerging technology full of challenges. Ann Pharm Fr 2021; 79:107-18. doi: 10.1016/j.pharma.2020.08.007 [Crossref] [ Google Scholar]
- Deshmane S, Kendre P, Mahajan H, Jain S. Stereolithography 3D printing technology in pharmaceuticals: a review. Drug Dev Ind Pharm 2021; 47:1362-72. doi: 10.1080/03639045.2021.1994990 [Crossref] [ Google Scholar]
- Moroni S, Khorshid S, Aluigi A, Tiboni M, Casettari L. Poly(3-hydroxybutyrate): A potential biodegradable excipient for direct 3D printing of pharmaceuticals. Int J Pharm 2022; 623:121960. doi: 10.1016/j.ijpharm.2022.121960 [Crossref] [ Google Scholar]
- Weng T, Zhang W, Xia Y, Wu P, Yang M, Jin R. 3D bioprinting for skin tissue engineering: Current status and perspectives. J Tissue Eng 2021; 12:20417314211028574. doi: 10.1177/20417314211028574 [Crossref] [ Google Scholar]