Bioimpacts. 16:33050.
doi: 10.34172/bi.33050
Editorial
Pharmacists in modern primary care and management of diseases: an evidence-based perspective on emerging technologies
Jaleh Barar Conceptualization, Writing – original draft, Writing – review & editing, 1 
Yadollah Omidi Conceptualization, Writing – original draft, Writing – review & editing, 1, *
Author information:
1Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
Abstract
Modern healthcare demands warrant the reconceptualization of pharmaceutical practitioners as primary caregivers capable of addressing contemporary medical challenges. Their specialized knowledge in molecular therapeutics, computational medicine tools, and physiological surveillance technologies uniquely qualifies them to oversee complicated treatment protocols for cutting-edge interventions, including genomic modifications and targeted biological agents. Historical success in managing long-term metabolic and cardiovascular conditions establishes credibility for supervising precision medicine applications. Digital innovations (e.g., remote consultation systems, algorithmic forecasting, and distributed ledger prescription tracking) enhance their capacity to coordinate fragmented services while responding to infectious outbreaks and polypharmacy challenges in elderly populations. This evolution promises decreased emergency admissions, improved therapeutic compliance, and more cost-effective care delivery. Regulatory reform must eliminate practice limitations, enabling these accessible professionals to address population health requirements fully.
Graphical Abstract
Keywords: Pharmaceutical care expansion, Precision medicine, Digital health technology, Advanced therapeutics, Interprofessional collaboration, Healthcare policy reform
Copyright and License Information
© 2026 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None to be declared.
Introduction
Persistent medical conditions constitute a paramount concern for global health systems, accounting for a disproportionate share of healthcare resources and contributing substantially to population disease burden. Hacker projects that worldwide expenditures related to chronic illness will reach an astounding $47 trillion by 2030,1 while within American borders, approximately 90% of the $4.9 trillion spent annually on healthcare addresses chronic and behavioral health disorders.2 This enormous financial strain, coupled with dwindling numbers of primary care practitioners and an increasingly elderly population with multifaceted medical requirements, demands novel strategies for delivering healthcare services. A particularly promising approach involves deeper incorporation of pharmacists into frontline care delivery, capitalizing on their sophisticated training in medication science, disease management protocols, and patient education to fill crucial voids in the healthcare infrastructure.
The metamorphosis of pharmacy from a predominantly product-dispensing occupation to one centered on holistic patient care has been facilitated through collaborative practice agreements (CPAs). These legal mechanisms authorize pharmacists to function alongside physicians in delivering designated patient care activities, encompassing medication regimen modifications, laboratory test ordering, and implementation of individualized lifestyle interventions.3 Sachdev and Goodlet outline four distinct frameworks for pharmacist prescriptive privileges across the United States, spanning from patient-centered collaborative prescribing via CPAs to class-based prescribing authority, with substantial interstate variation.4 The fragmented regulatory landscape in the United States seems to create significant barriers to uniform pharmacist practice advancement, contrasting sharply with more cohesive international models. While the four-tiered framework highlights progressive expansion of pharmacist autonomy, the state-by-state variation necessitates complex navigation of jurisdiction-specific regulations that can impede consistent care delivery and inter-state practice mobility. This stands in stark contrast to countries like the United Kingdom, where pharmacist independent prescribers possess full prescriptive authority following standardized national training and credentialing, enabling them to prescribe any medication within their competence area without collaborative agreements or physician co-signatures. The UK model, established through the Health and Social Care Act, eliminates many administrative barriers inherent in the CPA framework, allowing for more streamlined care delivery. These international differences highlight how regulatory infrastructure, rather than pharmacist capability, often determines the scope of advanced practice, with US pharmacists facing persistent legislative hurdles despite demonstrated clinical competency and positive patient outcomes in states with expanded authority. This heterogeneity mirrors the continuing transformation of pharmaceutical practice and the profession's trajectory toward achieving formal healthcare provider designation. This mini review highlights the key roles of pharmacists in primary care management intertwined with emerging technologies.
The scientific foundation validating pharmacist-directed chronic condition oversight is substantial and expanding continuously. Newman et al performed an umbrella review examining community pharmacist-initiated programs and discovered that pharmacists successfully enhanced clinical parameters across numerous persistent diseases, encompassing glucose metabolism disorders, lipid abnormalities, cardiovascular pathology, and pulmonary conditions.5 Similarly, an exhaustive systematic analysis by Greer et al commissioned by the Department of Veterans Affairs determined that pharmacist-directed chronic disease oversight yielded outcomes comparable to conventional care regarding resource consumption while potentially advancing physiologic target achievement.6 Rahayu and colleagues underscored that incorporating pharmacists into interprofessional healthcare units has demonstrated capacity to facilitate primary care accessibility and elevate patient outcomes across multiple care delivery dimensions.7
Within diabetes care, pharmacist contributions prove especially remarkable. Norton et al established that average hemoglobin A1c reductions reached 1.75% in collaborative pharmacist-physician models versus merely 0.16% in standard care cohorts across twelve months, representing a therapeutically meaningful difference in glucose regulation.8 McCarthy and Van documented comparably impressive findings in a Federally Qualified Health Center environment, where pharmacists possessing prescriptive authority attained statistically significant improvements including a 2.1% A1c decrease for type 2 diabetes patients.9 Additionally, Wagner et al found that individuals receiving pharmacist care demonstrated three to five-fold greater likelihood of achieving comprehensive diabetes quality benchmarks compared to those obtaining standard care.10 It has been shown that 52.84% of patients with inadequately controlled diabetes reached A1c concentrations below 9% following pharmacist-delivered medication therapy management in community health facilities, illustrating the scalability of these interventions across heterogeneous practice locations.11
Blood pressure control represents another domain where pharmacists have exhibited equivalent or superior results to conventional care paradigms. In a meta-analysis, Santschi and colleagues analyzed data from randomized controlled trials encompassing over 14,000 subjects and found that interventions led by pharmacists were associated with substantial decreases in both systolic and diastolic blood pressure levels.12 Through a randomized pragmatic investigation, it has been shown that pharmacist-physician collaborative medication management proved more efficacious in reducing blood pressure at both six and nine months relative to usual care.13 McCarthy and Van further substantiated these conclusions with data revealing a 29.7 mmHg systolic blood pressure decline among hypertensive individuals managed by pharmacists with prescriptive authorization.9 The uniformity of these observations across multiple investigations and environments furnishes persuasive validation for pharmacist participation in hypertension oversight.
Cardiovascular risk factor management in diabetic populations has similarly benefited from pharmacist involvement. In a 2012 systematic review and meta-analysis, Santschi et al demonstrated that pharmaceutical care interventions were associated with meaningful reductions in systolic blood pressure, total cholesterol levels, and LDL cholesterol concentrations in patients with diabetes.14 These concurrent improvements across multiple cardiovascular risk elements underscore the comprehensive character of pharmacist-directed care and its capacity to address the intricate, multidimensional requirements of patients with persistent conditions. Such multifaceted interventions prove particularly valuable considering that one in three adults globally manages multiple chronic conditions, which exponentially amplifies treatment complexity and healthcare expenditures.
In pulmonary disease oversight, particularly asthma, pharmacists have exhibited extraordinary capability to enhance clinical parameters and diminish disease exacerbations. In their 2021 meta-analytic study, Bridgeman and Wilken examined various interventions led by pharmacy professionals and found substantial decreases in acute exacerbation frequencies across asthma and COPD patient populations. These positive outcomes were observed when pharmaceutical care initiatives included hands-on instruction of proper inhalation methods along with practice sessions using dummy inhaler devices.15 These interventions additionally reduced rescue medication utilization and improved both inhaler technique and treatment compliance. Armour et al performed a systematic review confirming that pharmacists exert positive influence on various clinical asthma outcomes, including symptom management and prevention of future exacerbations.16 García-Cárdenas et al demonstrated through a cluster randomized trial that pharmacist interventions emphasizing appropriate medication utilization and tailored to patients' current asthma control status significantly enhanced asthma control scores, particularly among patients with insufficiently controlled asthma at baseline.17
The evidence validating expanded pharmacist roles extends beyond clinical parameters to encompass broader healthcare system advantages. The American College of Managed Care Pharmacy position statement emphasizes that when pharmacists receive recognition as provider members of the healthcare team, patient outcomes improve, patients report elevated satisfaction rates, and overall healthcare costs diminish.2 A systematic review by Marupuru and colleagues examined how pharmacist-delivered medication therapy management affected health outcomes in individuals diagnosed with diabetes, high blood pressure, or elevated cholesterol levels, revealing meaningful statistical enhancements in patient health measures for each of the three medical conditions studied.18 These findings support the economic justification for integrating pharmacists into primary care teams, as improved disease control can lead to reduced hospitalizations, emergency department visits, and long-term complications.
The movement toward formal provider status recognition for pharmacists represents the natural progression of this evidence base. Cernasev et al discuss the evolution from collaborative practice agreements toward comprehensive provider status, noting that such recognition would enable pharmacists to receive reimbursement under Medicare Part B for delivering essential healthcare services to patients.19 This policy modification would not only acknowledge the clinical contributions pharmacists make but also ensure the sustainability and scalability of pharmacist-led services across diverse healthcare settings. Since nearly nine out of ten American citizens live in close proximity to a local drugstore, granting pharmacy professionals enhanced medication-ordering powers and acknowledging them as healthcare practitioners would substantially boost the availability of basic medical care, especially for populations with limited medical support.
Digital innovations are reshaping the landscape of pharmacy practice, creating pathways for pharmacists to extend their clinical influence far beyond conventional practice boundaries. Virtual care delivery platforms have proven particularly valuable in bridging geographical barriers that traditionally limited access to pharmaceutical expertise. In this line, artificial intelligence (AI)-assisted pharmacogenomics has emerged as a particularly promising application, enabling personalized medicine implementation at unprecedented scale. These systems analyze patients' genetic profiles alongside clinical data to predict individual responses to specific medications, empowering pharmacists to make evidence-based recommendations for drug selection and dosing optimization.20,21 Recent implementation studies have shown that pharmacist-driven pharmacogenomic services, supported by AI algorithms, substantially improved therapeutic outcomes in cardiovascular disease management,22 and reduced trial-and-error prescribing in mental health treatment significantly.23,24 This technology democratizes precision medicine, making sophisticated genetic-based treatment optimization accessible in community pharmacy settings rather than limiting it to specialized academic centers.
Algorithmic forecasting and predictive analytics further enhance pharmacists' ability to intervene proactively in chronic disease management. Machine learning algorithms can now identify patients at high risk for medication non-adherence, disease exacerbations, or emergency department visits by analyzing patterns in refill histories, laboratory values, and social determinants of health. Recent studies revealed that pharmacists utilizing AI-driven risk stratification tools achieved a meaningful reduction in diabetes-related hospitalizations through timely preventive interventions.25-28 These systems essentially provide pharmacists with a "clinical radar," detecting subtle warning signs that would otherwise remain invisible until after adverse outcomes occur. Blockchain-based prescription tracking systems are revolutionizing medication safety and supply chain integrity while simultaneously expanding pharmacists' surveillance capabilities. These distributed ledger technologies create immutable records of medication dispensing, enabling real-time detection of prescription forgery, doctor shopping behaviors, and supply chain compromises.29-31 It has been demonstrated that blockchain implementation in integrated healthcare systems reduced opioid misuse and eliminated counterfeit medication infiltration entirely in pilot programs.32 Beyond security benefits, these systems provide pharmacists with comprehensive medication histories across multiple providers and pharmacies, facilitating more informed clinical interventions and eliminating dangerous information gaps that plague fragmented healthcare delivery.
Wearable biosensors,33,34 and Internet of Medical Things (IoMT) devices35-37 create continuous physiological monitoring streams that transform pharmacists from reactive problem-solvers into proactive health optimizers. When integrated with AI analytics platforms, data from continuous glucose monitors, blood pressure cuffs, and cardiac rhythm sensors enable pharmacists to adjust medication regimens based on real-world physiological responses rather than relying solely on periodic clinic measurements. Remarkably, pharmacist-managed remote monitoring programs utilizing AI-analyzed biosensor data reduced heart failure readmissions significantly and improved glycemic control in type 2 diabetes patients by an average of 1.2% HbA1c reduction beyond standard care. These digital innovations collectively enable a fundamental shift from episodic, reactive pharmaceutical care to continuous, predictive, and personalized medication management. The synergy between AI-assisted systems and pharmacist expertise creates a powerful paradigm where technology handles data-intensive pattern recognition while pharmacists apply clinical judgment, therapeutic knowledge, and patient-centered communication skills that remain uniquely human capabilities. This technological augmentation does not replace pharmacist expertise but rather amplifies it, enabling individual pharmacists to deliver sophisticated, evidence-based care to larger patient populations with greater precision than previously achievable. The integration of AI into pharmaceutical practice represents a transformative advancement in delivering patient-centered care, enabling pharmacists to optimize therapeutic outcomes through precision medicine and real-time monitoring capabilities. AI-driven technologies are revolutionizing drug delivery systems, from the design of intelligent nanocarriers for ocular therapeutics to the development of personalized microneedle-based biosensing devices that enable autonomous drug administration with minimal human intervention.38,39 These innovations empower pharmacists to move beyond traditional dispensing roles toward comprehensive medication management, utilizing AI algorithms to predict drug release kinetics, optimize formulation parameters for individual patient needs, and design smart delivery platforms that respond to physiological changes in real time.40 Furthermore, AI-powered wearable biosensors integrated with machine learning enable continuous monitoring of therapeutic biomarkers and disease progression, allowing hospital/clinical pharmacists to provide proactive interventions for conditions ranging from Parkinson's disease to chronic wound management.41,42 This technological convergence facilitates the transition from empirical, trial-and-error approaches to data-driven, evidence-based pharmaceutical care that accounts for patient-specific variability in drug response and disease presentation. Beyond individualized therapy optimization, AI integration significantly enhances clinical decision-making and patient safety within pharmaceutical practice. Point-of-care sensor systems equipped with AI algorithms enable pharmacists to conduct rapid, accurate detection of therapeutic drugs in blood samples with detection limits substantially below therapeutic thresholds, facilitating precise dosage adjustments and preventing adverse events.43,44 Machine learning models analyzing complex datasets from electronic health records, genomic profiles, and wearable devices allow pharmacists to predict disease trajectories, identify patients at risk for medication-related problems, and recommend optimized treatment strategies that reduce errors while improving resource utilization.45 The deployment of AI-enhanced detection systems also strengthens pharmaceutical surveillance capabilities, with gradient boosting algorithms achieving 99% accuracy in identifying antibiotic residues and supporting antimicrobial stewardship efforts.46 Additionally, the integration of AI with Internet of Medical Things platforms enables seamless coordination of home-based care and prehospital services, positioning pharmacists as key contributors to accessible, efficient healthcare delivery that extends beyond traditional practice settings.35 Taken all, these AI-driven innovations empower pharmacists to function as essential clinical decision-support partners, bridging technology and patient care to deliver safer, more effective, and equitable pharmaceutical services.
Research by Baldoni et al revealed that when pharmacists utilized telecommunication technologies to deliver services, patients demonstrated enhanced commitment to their medication regimens and experienced better health outcomes across various disease states.47 The rapid expansion of these remote consultation capabilities, particularly accelerated during recent public health emergencies, has validated the feasibility of pharmacists managing complex therapeutic regimens through digital channels. Simultaneously, computational intelligence systems are revolutionizing how medication-related decisions are made in clinical practice. According to Reddy et al, machine learning applications can detect potential medication conflicts, forecast unintended medication effects, and tailor drug selection to individual patient characteristics, thereby supporting pharmacists in delivering more precise therapeutic interventions.48 These sophisticated algorithms process extensive patient datasets to flag individuals who may be vulnerable to medication complications, allowing pharmacists to intervene preventively rather than reactively. The maturation of interconnected digital health information systems has similarly transformed interprofessional collaboration, with Berbakov et al reporting that when pharmacists gained comprehensive visibility into patient medical records, their capacity to make sound clinical judgments and detect medication issues improved substantially.49 Continuous monitoring technologies represent yet another frontier in pharmaceutical care delivery. A comprehensive evidence established that when pharmacists incorporated connected health devices and remote monitoring and telemanagement program into their practice models, patients with persistent medical conditions, especially those managing glucose metabolism disorders and elevated blood pressure, achieved superior therapeutic endpoints.50 These digital tools capture physiological parameters, treatment compliance patterns, and behavioral indicators in real-time, furnishing pharmacists with intelligence needed to fine-tune therapeutic strategies and transition care delivery from episodic intervention to sustained disease prevention.
Despite the considerable promise these technological advances hold for expanding pharmaceutical care delivery, multiple obstacles must be overcome to achieve widespread implementation. It has been documented that pharmacists face significant hurdles, including insufficient preparation for using new technologies, difficulties embedding digital tools into existing workflows, apprehension regarding patient information security, and uncertain compensation mechanisms for services delivered through technology platforms.51 Concerns about equitable access are particularly pressing, as populations with limited digital literacy or inadequate internet connectivity may be further disadvantaged if technology deployment proceeds without intentional attention to inclusive design principles. Advancing the field will require rigorous investigation into how these innovations can be successfully woven into varied practice environments while preserving the interpersonal connections and clinical judgment that distinguish exceptional pharmaceutical care. The simultaneous expansion of pharmacists' clinical responsibilities and the proliferation of healthcare technologies presents a unique moment to fundamentally redesign primary care delivery systems. When pharmacists harness virtual consultation platforms, computational intelligence, integrated health information networks, continuous monitoring capabilities, and software-based therapeutic interventions, their capacity to serve larger populations more effectively multiplies exponentially. These digital tools serve not as substitutes for pharmaceutical expertise and therapeutic relationships, but as force multipliers that enable pharmacists to deliver individualized, scientifically-grounded care to substantially more patients. As health systems worldwide struggle with inadequate access, inconsistent quality, and unsustainable costs, pharmacist services enhanced by technology offer a realistic solution for achieving more productive, fair, and patient-focused care delivery. The scientific evidence demonstrating both the therapeutic value of pharmacist-directed services and the transformative potential of digital health innovations is now robust and convincing. What remains is for policy architects, payment system designers, and practice leaders to synchronize their efforts in removing impediments and creating conditions that allow pharmacists to fully contribute their unique capabilities toward improving population health.
As concluding remarks, the incorporation of pharmacists into primary care and clinical services represents a paradigm transformation with capacity to substantially enhance healthcare delivery and patient outcomes. The extensive evidence base establishes that pharmacists can independently oversee common chronic conditions such as hypertension, diabetes, and dyslipidemia, frequently achieving outcomes equivalent to or surpassing those of traditional provider models. Through collaborative practice agreements, pharmacists can optimize medication therapy, provide continuous patient education, implement evidence-based interventions, and address barriers to medication adherence in ways that complement and extend the capabilities of overburdened primary care systems. As healthcare systems worldwide grapple with the escalating burden of chronic disease, constrained resources, and workforce shortages, the full integration of pharmacists as recognized providers offers a practical, evidence-based solution. Fig. 1 illustrates the pharmacists’ involvements in technology-based diseases management.
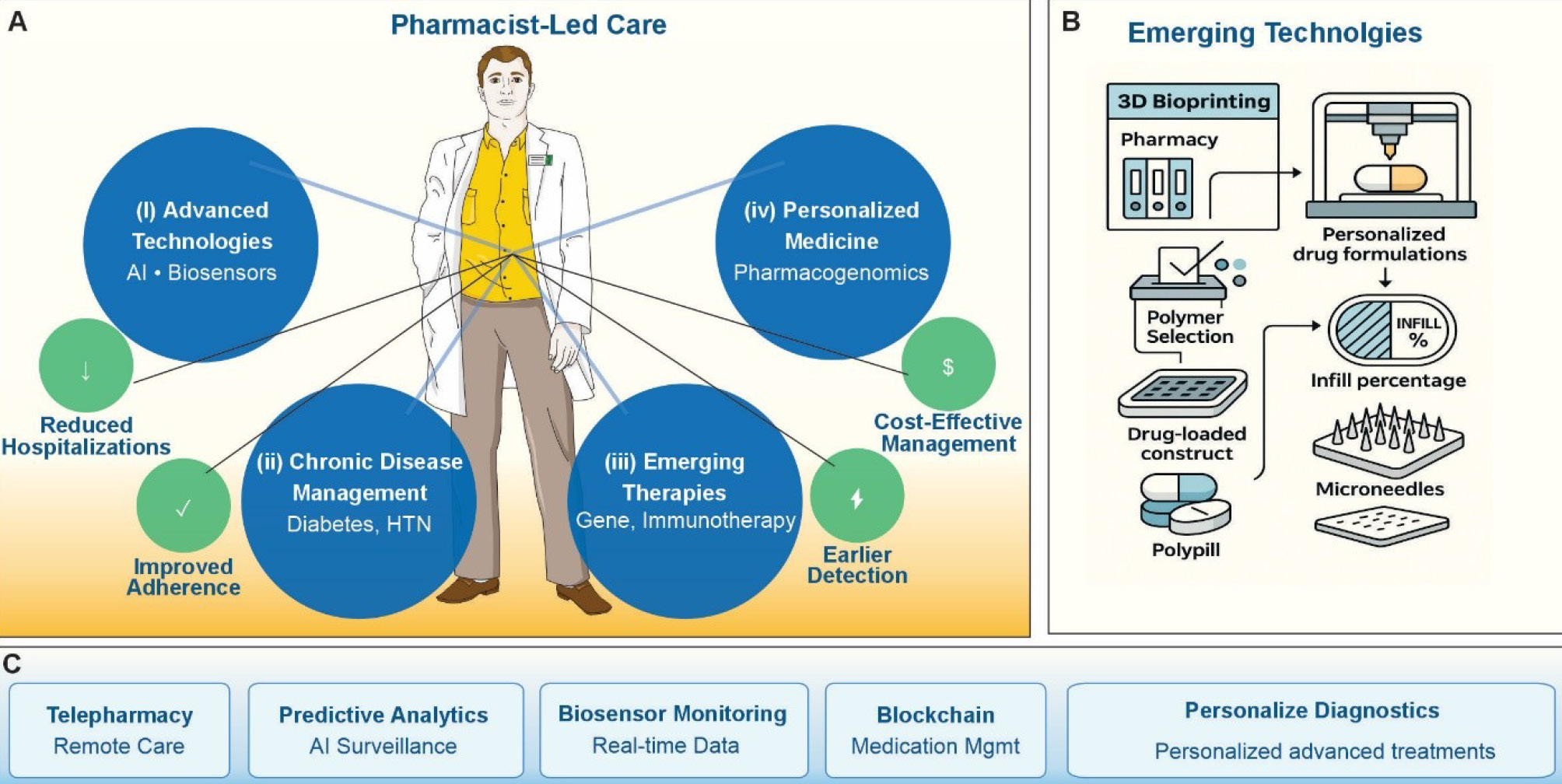
Fig. 1.
The conceptual framework illustration for the integration of pharmacist-led care with emerging healthcare technologies and diseases management. (A) The pivotal role of pharmacy practitioners in coordinating four key domains of modern pharmaceutical practice as (i) Advanced Technologies (AI and biosensors), (ii) Chronic Disease Management (diabetes and hypertension (HTN)), (iii) Emerging Therapies (gene therapy and immunotherapy), and (iv) Personalized Medicine (pharmacogenomics). Green circles highlight patient-centered outcomes including reduced hospitalizations, improved medication adherence, cost-effective management, and earlier disease detection. (B) The 3D bioprinting workflow for personalized pharmaceutical manufacturing, demonstrating the progression from pharmacy inventory through polymer selection and drug-loaded construct development to final dosage. forms including customized infill percentages, microneedle arrays, and polypill formulations. (C) The digital health platforms: telepharmacy for remote care delivery, predictive analytics with AI surveillance, biosensor monitoring for real-time patient data, blockchain for medication management, and personalized diagnostics for individualized treatment planning. This integrated model emphasizes the expanding scope of pharmacy practice in delivering precision medicine through technological innovation
.
The conceptual framework illustration for the integration of pharmacist-led care with emerging healthcare technologies and diseases management. (A) The pivotal role of pharmacy practitioners in coordinating four key domains of modern pharmaceutical practice as (i) Advanced Technologies (AI and biosensors), (ii) Chronic Disease Management (diabetes and hypertension (HTN)), (iii) Emerging Therapies (gene therapy and immunotherapy), and (iv) Personalized Medicine (pharmacogenomics). Green circles highlight patient-centered outcomes including reduced hospitalizations, improved medication adherence, cost-effective management, and earlier disease detection. (B) The 3D bioprinting workflow for personalized pharmaceutical manufacturing, demonstrating the progression from pharmacy inventory through polymer selection and drug-loaded construct development to final dosage. forms including customized infill percentages, microneedle arrays, and polypill formulations. (C) The digital health platforms: telepharmacy for remote care delivery, predictive analytics with AI surveillance, biosensor monitoring for real-time patient data, blockchain for medication management, and personalized diagnostics for individualized treatment planning. This integrated model emphasizes the expanding scope of pharmacy practice in delivering precision medicine through technological innovation
Modern healthcare systems still continue to face unprecedented challenges from emerging infectious diseases, complex metabolic disorders, and rapidly advancing therapeutic technologies. Pharmacists, with expanded provider status recognition, are uniquely positioned to address these challenges through patient-centered care delivery. Their advanced training in pharmacogenomics, AI-assisted medication optimization, and real-time biosensor monitoring enables them to lead integrated care teams managing intricate therapeutic regimens for conditions ranging from gene therapy complications to antibiotic-resistant infections.
The foundation for this expanded role rests on pharmacists' proven expertise in chronic disease management. Clinical outcomes data demonstrate superior results in diabetes control, hypertension management, cardiovascular risk reduction, and respiratory disease optimization. This track record provides a solid basis for navigating increasingly personalized medicine approaches, including CRISPR-based treatments, nanopharmaceuticals, and adaptive biologic therapies. Furthermore, emerging technologies amplify pharmacist capabilities in primary care settings. Telepharmacy platforms extend access to underserved populations. Predictive analytics and continuous monitoring systems (e.g., tracking metrics from glucose levels to blood pressure) enable proactive intervention before complications arise. Blockchain-based medication management systems ensure accuracy and coordination across fragmented healthcare networks. These tools position pharmacists to respond rapidly to pandemic threats, optimize complex multi-drug regimens for aging populations with multiple comorbidities, and coordinate seamlessly with other providers. Concludingly, pharmacist-led interventions reduce hospitalizations, improve medication adherence through smart delivery systems, enable earlier detection of adverse effects via AI surveillance, and provide cost-effective management of both chronic and acute conditions. These outcomes become increasingly critical as pharmaceutical innovation outpaces traditional care delivery models. Healthcare systems can no longer afford to underutilize this highly trained, accessible workforce. Removing barriers to full pharmacist practice authority addresses critical gaps in care access and quality while reducing overall healthcare costs. Both policymakers and healthcare leaders must act decisively to integrate pharmacists fully into interprofessional teams, ensuring that their expertise contributes meaningfully to meeting the diverse healthcare needs of modern populations.
Competing Interests
The authors declare no conflict of interest.
Ethical Approval
Not applicable.
Declaration of AI-assisted Tools in the Writing Procedure
The authors would like to declare that the fully licensed Anthropic's Claude AI has bee used to enhance the clarity of the language and the readability of the article.
Acknowledgements
The authors would like to acknowledge the Nova Southeastern University support.
References
- Hacker K. The Burden of Chronic Disease. Mayo Clin Proc Innov Qual Outcomes 2024; 8:112-9. doi: 10.1016/j.mayocpiqo.2023.08.005 [Crossref] [ Google Scholar]
- Academy of Managed Care Pharmacy. Provider Status for Pharmacists: Managed Care Practice Issues; Legislative and Regulatory Position Statement. 2023; Available from: https://www.amcp.org/legislative-regulatory-position/provider-status-pharmacists.
- Centers for Disease Control and Prevention. Collaborative Practice Agreements and Pharmacists' Patient Care Services: A Resource for Pharmacists. 2013; Available from: https://www.cdc.gov/high-blood-pressure/media/pdfs/2024/04/Translational_Tools_Pharmacists.pdf.
- Sachdev G, Kliethermes MA, Vernon V, Leal S, Crabtree G. Current status of prescriptive authority by pharmacists in the United States. J Am Coll Clin Pharm 2020; 3:807-17. doi: 10.1002/jac5.1245 [Crossref] [ Google Scholar]
- Newman TV, San-Juan-Rodriguez A, Parekh N, Swart ECS, Klein-Fedyshin M, Shrank WH. Impact of community pharmacist-led interventions in chronic disease management on clinical, utilization, and economic outcomes: An umbrella review. Res Social Adm Pharm 2020; 16:1155-65. doi: 10.1016/j.sapharm.2019.12.016 [Crossref] [ Google Scholar]
- Greer N, Bolduc J, Geurkink E, Koeller E, Rector T, Olson K, et al. VA Evidence-based Synthesis Program Reports. Pharmacist-Led Chronic Disease Management: A Systematic Review of Effectiveness and Harms Compared to Usual Care. Washington (DC): Department of Veterans Affairs (US); 2015.
- Rahayu SA, Widianto S, Defi IR, Abdulah R. Role of pharmacists in the interprofessional care team for patients with chronic diseases. J MultidiscipHealthc 2021; 14:1701-10. doi: 10.2147/JMDH.S309938 [Crossref] [ Google Scholar]
- Norton MC, Haftman ME, Buzzard LN. Impact of Physician-Pharmacist Collaboration on Diabetes Outcomes and Health Care Use. J Am Board Fam Med 2020; 33:745-53. doi: 10.3122/jabfm.2020.05.200044 [Crossref] [ Google Scholar]
- McCarthy C, Thomas Bateman Jr M. Impact of pharmacist-led chronic disease management in a Federally Qualified Health Center. J Am Coll Clin Pharm 2022; 5:1263-77. doi: 10.1002/jac5.1720 [Crossref] [ Google Scholar]
- Wagner TD, Dixon DL, Shin Y, Dozmorov M, Musselman KT, Buffington TM. Impact of pharmacist-physician collaborative care on hemoglobin A1c and blood pressure quality measure achievement in primary care. J Manag Care Spec Pharm 2025; 31:565-77. doi: 10.18553/jmcp.2025.31.6.565 [Crossref] [ Google Scholar]
- Rodis JL, Sevin A, Awad MH, Porter B, Glasgow K, Hornbeck Fox C. Improving Chronic Disease Outcomes Through Medication Therapy Management in Federally Qualified Health Centers. J Prim Care Community Health 2017; 8:324-31. doi: 10.1177/2150131917701797 [Crossref] [ Google Scholar]
- Santschi V, Chiolero A, Colosimo AL, Platt RW, Taffé P, Burnier M. Improving blood pressure control through pharmacist interventions: a meta-analysis of randomized controlled trials. J Am Heart Assoc 2014; 3:e000718. doi: 10.1161/jaha.113.000718 [Crossref] [ Google Scholar]
- Hirsch JD, Steers N, Adler DS, Kuo GM, Morello CM, Lang M. Primary care-based, pharmacist-physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther 2014; 36:1244-54. doi: 10.1016/j.clinthera.2014.06.030 [Crossref] [ Google Scholar]
- Santschi V, Chiolero A, Paradis G, Colosimo AL, Burnand B. Pharmacist interventions to improve cardiovascular disease risk factors in diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2012; 35:2706-17. doi: 10.2337/dc12-0369 [Crossref] [ Google Scholar]
- Bridgeman MB, Wilken LA. Essential Role of Pharmacists in Asthma Care and Management. J Pharm Pract 2021; 34:149-62. doi: 10.1177/0897190020927274 [Crossref] [ Google Scholar]
- Garcia-Cardenas V, Armour C, Benrimoj SI, Martinez-Martinez F, Rotta I, Fernandez-Llimos F. Pharmacists' interventions on clinical asthma outcomes: a systematic review. Eur Respir J 2016; 47:1134-43. doi: 10.1183/13993003.01497-2015 [Crossref] [ Google Scholar]
- García-Cárdenas V, Sabater-Hernández D, Kenny P, Martínez-Martínez F, Faus MJ, Benrimoj SI. Effect of a pharmacist intervention on asthma control A cluster randomised trial. Respir Med 2013; 107:1346-55. doi: 10.1016/j.rmed.2013.05.014 [Crossref] [ Google Scholar]
- Marupuru S, Roether A, Guimond AJ, Stanley C, Pesqueira T, Axon DR. A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia. Healthcare (Basel) 2022; 10:1207. doi: 10.3390/healthcare10071207 [Crossref] [ Google Scholar]
- Cernasev A, Aruru M, Clark S, Patel K, DiPietro Mager N, Subramaniam V. Empowering Public Health Pharmacy Practice-Moving from Collaborative Practice Agreements to Provider Status in the US. Pharmacy (Basel) 2021; 9:49. doi: 10.3390/pharmacy9010057 [Crossref] [ Google Scholar]
- Haga SB. Artificial intelligence, medications, pharmacogenomics, and ethics. Pharmacogenomics 2024; 25:611-22. doi: 10.1080/14622416.2024.2428587 [Crossref] [ Google Scholar]
- Simpson MD, Qasim HS. Clinical and Operational Applications of Artificial Intelligence and Machine Learning in Pharmacy: A Narrative Review of Real-World Applications. Pharmacy (Basel) 2025; 13:41. doi: 10.3390/pharmacy13020041 [Crossref] [ Google Scholar]
- Al-Maini M, Maindarkar M, Kitas GD, Khanna NN, Misra DP, Johri AM. Artificial intelligence-based preventive, personalized and precision medicine for cardiovascular disease/stroke risk assessment in rheumatoid arthritis patients: a narrative review. Rheumatol Int 2023; 43:1965-82. doi: 10.1007/s00296-023-05415-1 [Crossref] [ Google Scholar]
- Rahman MA, Victoros E, Davis R, Duaa T, Shanjana Y, Islam MR. Use of Artificial Intelligence in Mental Healthcare, Health Psychology, and Related Research: A Narrative Review to Address Challenges and Opportunities. Health Sci Rep 2025; 8:e71595. doi: 10.1002/hsr2.71595 [Crossref] [ Google Scholar]
- Rahman MA, Victoros E, Ernest J, Davis R, Shanjana Y, Islam MR. Impact of Artificial Intelligence (AI) Technology in Healthcare Sector: A Critical Evaluation of Both Sides of the Coin. Clin Pathol 2024; 17:2632010x241226887. doi: 10.1177/2632010x241226887 [Crossref] [ Google Scholar]
- Messina R, Fantini MP, Lodi M, Di Bartolo P, Chattat R, Lenzi J. Patient-Reported Outcome Measures in Adults with Type 2 Diabetes-With a Focus on Older Populations: An AI-Assisted Rapid Review of Use and Implementation in Clinical and Organizational Practice. Healthcare (Basel) 2025; 13:2840. doi: 10.3390/healthcare13222840 [Crossref] [ Google Scholar]
- Deng M, Yang R, Zheng X, Deng Y, Jiang J. Artificial intelligence in diabetes care: from predictive analytics to generative AI and implementation challenges. Front Endocrinol (Lausanne) 2025; 16:1620132. doi: 10.3389/fendo.2025.1620132 [Crossref] [ Google Scholar]
- Zhou L, Gupta BB, Gaurav A, Attar RW, Alhomoud A, Arya V. AI-optimized GRU-based self-attention model for predictive diabetes staging in IoT healthcare 50. Sci Rep 2025; 16:307. doi: 10.1038/s41598-025-29674-z [Crossref] [ Google Scholar]
- Ben Lafqih M, Ait Lahbib F, Boutahar K, Azargui H, Elfatimy R, Motaib I. Assessing the quality and guideline-concordance of AI-powered chatbots in nutritional management of diabetes. Diabetes MetabSyndr 2025; 19:103355. doi: 10.1016/j.dsx.2025.103355 [Crossref] [ Google Scholar]
- Omidian H, Omidi Y. Blockchain in pharmaceutical life cycle management. Drug Discov Today 2022; 27:935-8. doi: 10.1016/j.drudis.2022.01.018 [Crossref] [ Google Scholar]
- Omidian H, Omidi Y. Drug counterfeiting and decentralized whistleblowers. Drug Discov Today 2022; 27:103335. doi: 10.1016/j.drudis.2022.08.003 [Crossref] [ Google Scholar]
- Omidian H, Razmara J, Parvizpour S, Tabrizchi H, Masoudi-Sobhanzadeh Y, Omidi Y. Tracing drugs from discovery to disposal. Drug Discov Today 2023; 28:103538. doi: 10.1016/j.drudis.2023.103538 [Crossref] [ Google Scholar]
- Gonzales A, Smith SR, Dullabh P, Hovey L, Heaney-Huls K, Robichaud M. Potential Uses of Blockchain Technology for Outcomes Research on Opioids. JMIR Med Inform 2021; 9:e16293. doi: 10.2196/16293 [Crossref] [ Google Scholar]
- Wu KY, Su ME, Kim Y, Nguyen L, Marchand M, Tran SD. Wearable biosensors: A comprehensive overview. Prog Mol Biol Transl Sci 2025; 215:101-54. doi: 10.1016/bs.pmbts.2025.05.011 [Crossref] [ Google Scholar]
- Ganesan M, Devi RK, Wang CL, Lin YC, Lin WC, Lin SF. From Lab to Body: Advanced Electrochemical Biosensors for Illicit Drug Detection via Nanomaterials, AI, and Wearable Tech. ACS Sens 2025; 10:9153-82. doi: 10.1021/acssensors.5c02479 [Crossref] [ Google Scholar]
- Seth M, Jalo H, Högstedt Å, Medin O, Sjöqvist BA, Candefjord S. Technologies for Interoperable Internet of Medical Things Platforms to Manage Medical Emergencies in Home and Prehospital Care: Scoping Review. J Med Internet Res 2025; 27:e54470. doi: 10.2196/54470 [Crossref] [ Google Scholar]
- Mitchell Tan K, Zandi A, Tavakolian K, Wung SF. Point-of-Care Sensors and Medical Internet-of-Things Technologies to Manage Catheter-Associated Urinary Tract Infections in the Intensive Care Unit. Crit Care Nurs Clin North Am 2025; 37:327-45. doi: 10.1016/j.cnc.2025.02.005 [Crossref] [ Google Scholar]
- Alshehri D, Noman N, Chiong R, Miah SJ, Sverdlov AL, Ngo DT. Factors influencing the adoption of Internet of Medical Things for remote patient monitoring: A systematic literature review. Comput Biol Med 2025; 192:110142. doi: 10.1016/j.compbiomed.2025.110142 [Crossref] [ Google Scholar]
- Biswas AA, Dhondale MR, Agrawal AK, Serrano DR, Mishra B, Kumar D. Advancements in microneedle fabrication techniques: artificial intelligence assisted 3D-printing technology. Drug DelivTransl Res 2024; 14:1458-79. doi: 10.1007/s13346-023-01510-9 [Crossref] [ Google Scholar]
- Srivastava V, Yadav P, Yadav A, Parashar P. Artificial Intelligence in Ocular Drug Delivery: Precision Drug Delivery's New Horizon. AAPS PharmSciTech 2025; 27:55. doi: 10.1208/s12249-025-03271-9 [Crossref] [ Google Scholar]
- Aundhia C, Parmar G, Talele C, Shah N, Talele D. Impact of Artificial Intelligence on Drug Development and Delivery. Curr Top Med Chem 2025; 25:1165-84. doi: 10.2174/0115680266324522240725053634 [Crossref] [ Google Scholar]
- Ileșan RR, Cordoș CG, Mihăilă LI, Fleșar R, Popescu AS, Perju-Dumbravă L, et al. Proof of Concept in Artificial-Intelligence-Based Wearable Gait Monitoring for Parkinson's Disease Management Optimization. Biosensors (Basel) 2022; 12. doi: 10.3390/bios12040189.
- Khadeeja Thanha KP, Ayisha Sana P, Ajesh JS, Naseef PP, Tharayil H, Lubaib P. Advanced smart bioelectronics for wound healing: biosensing, drug delivery, and artificial intelligence. Int J Pharm 2025; 684:126098. doi: 10.1016/j.ijpharm.2025.126098 [Crossref] [ Google Scholar]
- Wei Q, Zhou L, Sun J, Wu G, Gong S, Gao Z. Rapid detection of drugs in blood using "molecular hook" surface-enhanced Raman spectroscopy and artificial intelligence technology for clinical applications. BiosensBioelectron 2025; 267:116855. doi: 10.1016/j.bios.2024.116855 [Crossref] [ Google Scholar]
-
Kovur P, Kovur KM, Rayat DY, Wishart DS. POC Sensor Systems and Artificial Intelligence-Where We Are Now and Where We Are Going? Biosensors (Basel) 2025; 15. doi: 10.3390/bios15090589.
- Fahim YA, Hasani IW, Kabba S, Ragab WM. Artificial intelligence in healthcare and medicine: clinical applications, therapeutic advances, and future perspectives. Eur J Med Res 2025; 30:848. doi: 10.1186/s40001-025-03196-w [Crossref] [ Google Scholar]
-
Venkateswaramurthy N, Chitra Thara S, Vidhya Lekshmi K, Singh S. Artificial Intelligence-Powered Detection Systems for Antibiotic Residues In Food and The Environment: A Mini Review With Special Focus on Milk Products and Environmental Matrices Analysis. Recent Adv Food Nutr Agric 2025. doi: 10.2174/012772574x388015250901211939.
-
Baldoni S, Amenta F, Ricci G. Telepharmacy Services: Present Status and Future Perspectives: A Review. Medicina (Kaunas) 2019; 55. doi: 10.3390/medicina55070327.
- Reddy S, Allan S, Coghlan S, Cooper P. A governance model for the application of AI in health care. J Am Med Inform Assoc 2020; 27:491-7. doi: 10.1093/jamia/ocz192 [Crossref] [ Google Scholar]
- Berbakov ME, Hoffins EL, Stone JA, Gilson AM, Chladek JS, Watterson TL. Adapting a community pharmacy intervention to improve medication safety. J Am Pharm Assoc (2003) 2024; 64:159-68. doi: 10.1016/j.japh.2023.11.009 [Crossref] [ Google Scholar]
- Stulock R, Montgomery J, Parker M, Soric A, Zeleznikar E. Pharmacist involvement in a comprehensive remote monitoring and telemanagement program. Am J Health Syst Pharm 2022; 79:888-95. doi: 10.1093/ajhp/zxac025 [Crossref] [ Google Scholar]
- Hatem NAH. Advancing Pharmacy Practice: The Role of Intelligence-Driven Pharmacy Practice and the Emergence of Pharmacointelligence. Integr Pharm Res Pract 2024; 13:139-53. doi: 10.2147/IPRP.S466748 [Crossref] [ Google Scholar]