Bioimpacts. 16:33132.
doi: 10.34172/bi.33132
Editorial
Exaggerating the risks of vaccination is a dangerous health threat
Robert C. Speth 1, * 
Author information:
1Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, 3300 S. University Dr., Fort Lauderdale, FL 33328, USA
Abstract
Vaccine hesitancy and opposition lacking empirical support represent significant threats to public health, particularly when amplified by public health officials. This commentary provides evidence-based refutation of such anti-vaccine arguments, including (i) the robust epidemiological data demonstrating vaccine efficacy in reducing disease incidence, mortality, and transmission; (ii) the comprehensive safety surveillance systems (VAERS, VSD, CISA) that monitor adverse events and consistently demonstrate favorable risk-benefit profiles; (iii) the biological mechanisms underlying both vaccine-induced immunity and rare adverse events; and (iv) the distinction between temporal association and causation in adverse event reporting. Thus it can be deduced that flawed logic and falsifications have been used to misrepresent the risks of vaccination. This endangers the lives and well-being of people who are susceptible to the diseases that vaccines can effectively prevent.
Keywords: mRNA vaccines, Pfizer BioNTech and Moderna vaccine, SARS-CoV-2, Anti-vaxxers, Medical Fraud, History of vaccination and variolation
Copyright and License Information
© 2026 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
No funding was received for preparation of this manuscript.
Throughout the long history of vaccine development,1 legal issues have shaped critical milestones.2 Methodologically, systematic vaccine development has largely depended on evidence-based evaluation across all four generations of vaccines (Fig. 1e), followed by rigorous research activities. In this line, phase-dependent methodologies established by regulatory agencies, including the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA). The vaccine industry has invested heavily in the systematic progression from first-generation live attenuated vaccines to fourth-generation mRNA platforms, adhering to consistent investigational frameworks, despite the differences in technological advancements.3 In the US, meticulous regulations are followed in terms of vaccine development,4 with vaccine safety being the most important factor.5 Notably, vaccines in each generation underwent extensive laboratory and animal testing to establish proof-of-concept, immunogenicity, and preliminary safety profiles. The positive impacts of such activities were proven for vaccines to prevent COVID-19.6 For live attenuated vaccines, serial passage techniques in non-human hosts or cell culture systems achieved pathogen attenuation while maintaining immunogenic epitopes. Subunit vaccines required identification and isolation of protective antigens through epitope mapping and structural biology approaches. Third-generation DNA vaccines necessitated optimization of plasmid design, promoter selection, and transfection efficiency. Fourth-generation mRNA vaccines required the development of modified nucleosides (pseudouridine, N1-methylpseudouridine) to reduce innate immune activation and lipid nanoparticle formulations to enable intracellular delivery while protecting against ribonuclease degradation. In terms of clinical trial phases, all vaccine candidates progress through three mandatory clinical phases before licensure.6,7 Phase I trials (20-100 participants) establish safety, reactogenicity, and initial immunogenicity through dose-escalation studies. Phase II trials (100-500 participants) expand safety databases and determine optimal dosing schedules and immunological endpoints (e.g., antibody titers, neutralizing capacity, and T-cell responses measured via enzyme-linked immunospot (ELISPOT) or flow cytometry) to demonstrate efficacy. Phase III trials (10,000-50,000 + participants) employ randomized, double-blind, placebo-controlled designs to validate clinical efficacy against disease endpoints, with statistical power calculations ensuring adequate sample sizes to detect any adverse vaccine effects. For COVID-19 mRNA vaccines, Phase III trials enrolled over 40,000 participants each, with primary endpoints of laboratory-confirmed symptomatic infection occurring ≥ 7 days post-dose 2.7-10 Post-licensure surveillance is key to validating vaccine efficacy and safety. As a result, following regulatory approval, Phase IV pharmacovigilance of COVID-19 mRNA vaccines employed multiple complementary systems. Passive surveillance through the Vaccine Adverse Event Reporting System (VAERS), established in 1990, captured spontaneous adverse event reports from healthcare providers and patients.11 Active surveillance through the Vaccine Safety Datalink (VSD) utilized electronic health records from nine integrated healthcare organizations, enabling rapid sequential analysis for pre-specified adverse events of special interest. The Clinical Immunization Safety Assessment (CISA) project conducted detailed clinical investigations of complex cases. These systems collectively monitored millions of administered doses to detect rare adverse events (incidence < 1 per 100,000 doses) that Phase III trials lacked statistical power to identify. In terms of the evidence synthesis framework, for this manuscript, we conducted targeted literature searches in PubMed, Web of Science, and Cochrane Library databases using search terms, including "vaccine safety," "vaccine efficacy," "measles resurgence," "pertussis outbreak," "vaccine hesitancy," and "mRNA vaccine." Inclusion criteria comprised of (i) peer-reviewed epidemiological studies with sample sizes > 10,000 participants, (ii) meta-analyses and systematic reviews, (iii) official surveillance data from the Centers for Disease Control and Prevention (CDC), WHO, and EMA, and (iv) randomized controlled trials of licensed vaccines. We excluded preprints, opinion articles without primary data, and studies lacking appropriate control groups. Evidence quality was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework, with particular emphasis on large-scale cohort studies and randomized controlled trials (RCTs) providing high-certainty evidence for vaccine safety and effectiveness claims. Taken all together, with the complexity of vaccines, together with ethical and legal issues, the manufacturing and surveillance processes meet or surpass all the mandatory requirements for vaccine safety and efficacy.12
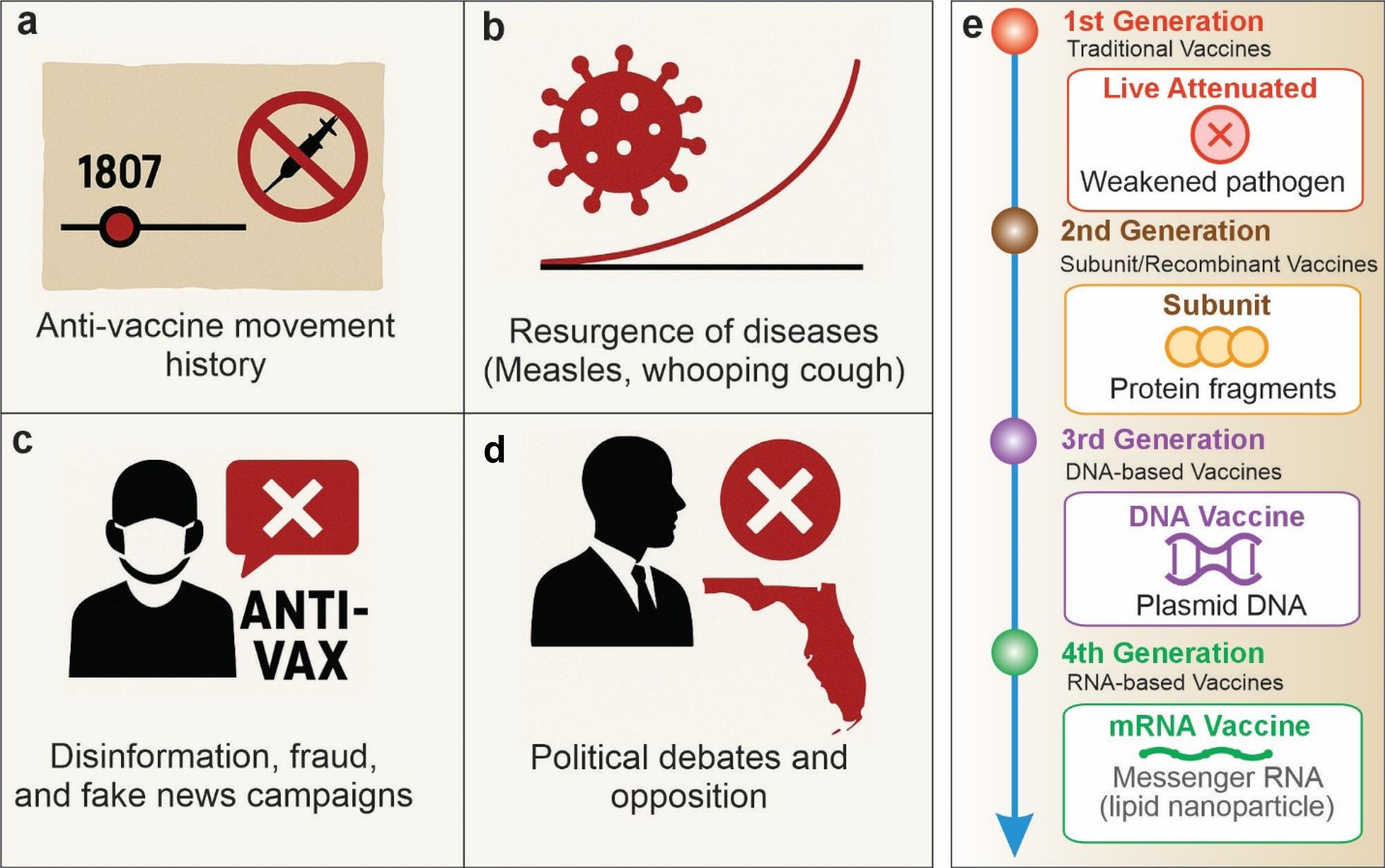
Fig. 1.
Evolution of the anti-vaccine movement and vaccine development. Panels a-d shows the antivaccine movement. (a) Early opposition in 1807; for details, readers are directed to see the following book.14 (b) Disease resurgence. (c) Modern disinformation. (d) Political exploitation. (e) Vaccine development through different generations. For details, readers are directed to see previous works in vaccine development.15-24 Emerging vaccines include (i) self-amplifying RNA (saRNA) vaccines are an evolution of mRNA technology where the RNA can replicate itself inside cells, potentially requiring much lower doses, (ii) nanoparticle vaccines arrange viral proteins on tiny particles that mimic the structure of viruses, creating very strong immune responses, and (iii) cell-based precision vaccines, including dendritic cell (DC) vaccines that are the most clinically advanced type of vaccines (Sipuleucel-T, Provenge®); tumor cell vaccines that use a patient's own cancer cells (autologous) or irradiated tumor cell lines (allogeneic) that are modified to enhance their immunogenicity, often by adding immune-stimulating molecules like GM-CSF, then administered to provoke anti-tumor immunity; neoantigen vaccines represent true precision medicine, where tumor DNA is sequenced to identify unique mutations (neoantigens) specific to that patient's cancer. These neoantigens are then used to create personalized vaccines, sometimes loaded onto dendritic cells or delivered via mRNA/peptides to activate T cells against those exact tumor targets; engineered cell-based platforms include modified immune cells that produce and present antigens, essentially becoming "living vaccine factories" within the body. Precision cell-based treatments also include FDA-approved chimeric antigen receptor T cell (CAR-T) therapies (e.g., Kymriah® (tisagenlecleucel) - CD19-targeting for B-cell leukemia/lymphoma; Yescarta® (axicabtagene ciloleucel) - CD19-targeting for lymphoma; Tecartus® (brexucabtagene autoleucel) - CD19-targeting for mantle cell lymphoma; Breyanzi® (lisocabtagene maraleucel) - CD19-targeting for lymphoma; Abecma® (idecabtagene vicleucel) - BCMA-targeting for multiple myeloma; Carvykti® (ciltacabtagene autoleucel) - BCMA-targeting for multiple myeloma).
.
Evolution of the anti-vaccine movement and vaccine development. Panels a-d shows the antivaccine movement. (a) Early opposition in 1807; for details, readers are directed to see the following book.14 (b) Disease resurgence. (c) Modern disinformation. (d) Political exploitation. (e) Vaccine development through different generations. For details, readers are directed to see previous works in vaccine development.15-24 Emerging vaccines include (i) self-amplifying RNA (saRNA) vaccines are an evolution of mRNA technology where the RNA can replicate itself inside cells, potentially requiring much lower doses, (ii) nanoparticle vaccines arrange viral proteins on tiny particles that mimic the structure of viruses, creating very strong immune responses, and (iii) cell-based precision vaccines, including dendritic cell (DC) vaccines that are the most clinically advanced type of vaccines (Sipuleucel-T, Provenge®); tumor cell vaccines that use a patient's own cancer cells (autologous) or irradiated tumor cell lines (allogeneic) that are modified to enhance their immunogenicity, often by adding immune-stimulating molecules like GM-CSF, then administered to provoke anti-tumor immunity; neoantigen vaccines represent true precision medicine, where tumor DNA is sequenced to identify unique mutations (neoantigens) specific to that patient's cancer. These neoantigens are then used to create personalized vaccines, sometimes loaded onto dendritic cells or delivered via mRNA/peptides to activate T cells against those exact tumor targets; engineered cell-based platforms include modified immune cells that produce and present antigens, essentially becoming "living vaccine factories" within the body. Precision cell-based treatments also include FDA-approved chimeric antigen receptor T cell (CAR-T) therapies (e.g., Kymriah® (tisagenlecleucel) - CD19-targeting for B-cell leukemia/lymphoma; Yescarta® (axicabtagene ciloleucel) - CD19-targeting for lymphoma; Tecartus® (brexucabtagene autoleucel) - CD19-targeting for mantle cell lymphoma; Breyanzi® (lisocabtagene maraleucel) - CD19-targeting for lymphoma; Abecma® (idecabtagene vicleucel) - BCMA-targeting for multiple myeloma; Carvykti® (ciltacabtagene autoleucel) - BCMA-targeting for multiple myeloma).
While anti-vaccination activists (anti-vaxxers) date back to 1807 (Fig. 1a), it has only been in the 21st century that anti-vaxxers have established a beachhead in their attack on the rational medical practice of vaccination against communicable diseases. Diseases such as measles and whooping cough that had been essentially wiped out by the end of the 20th century are now making a resurgence in areas, where vaccination rates have fallen below those needed to provide herd immunity (Fig. 1b). The main reason is that parents in these areas have fallen prey to the disinformation campaigns claiming vaccines do more harm than good. A recent survey indicates that 1 in 6 US parents are rejecting vaccine recommendations.13
Seemingly, among various factors, disinformation, fraud, fake news campaigns, and political opposition are the main driving forces in changing public trust in vaccination preventive/treatment modalities. (Fig.1c and 1d).
Historically, remarkable scientific evolution has been accomplished across the four vaccine generations (Fig. 1e). Edward Jenner (English physician, 1749-1823) pioneered the first successful vaccine, the so-called Jenner's cowpox vaccination, classified as a live heterologous vaccine. Later, the first-generation live attenuated vaccines (e.g., measles-mumps-rubella (MMR), and varicella vaccines) utilize weakened pathogens that replicate minimally while stimulating robust cellular and humoral immunity.
The resurgence of the anti-Vax movement of the 21st century can largely be traced to a now retracted 1998 study published in Lancet by the physician Andrew Wakefield et al25 claiming that the measles, mumps, and rubella (MMR) vaccine caused autism. Subsequent investigations of the paper that led to its retraction in 2010 included discovery of extensive data falsification, misrepresentation of the study population, and payments in excess of $500,000 from a group of lawyers representing parents of autistic children to make it appear that the MMR vaccine caused autism.26,27 For this egregious fraud, Andrew Wakefield and one other author of the paper had their medical licenses revoked. However, during the 12 years between publication and retraction of this paper, the belief that the MMR vaccine caused autism rivaled the power of Biblical beliefs and still resonates today. While there has been a multitude of studies that have refuted this claim,28 one compelling example is a 2019 Danish cohort study of 657,461 children (contributing 5,025,754 person-years). It found a slight reduction in risk of autism in vaccinated versus unvaccinated children (hazard ratio: 0.93; 95% CI: 0.85-1.02), even among high-risk subgroups.29 Meta-analyses encompassing over 1.2 million children consistently demonstrate no link between any vaccine and autism spectrum disorders.30 Surprisingly worse yet, the bogus MMR vaccine-autism link was generalized to all vaccines as also having dire adverse off-target effects, most recently with the development of mRNA vaccines for SARS-CoV-2 infections. Veterinarians are now reporting that pet owners are also resisting vaccination of their pets, including rabies vaccine.31 Ironically, many proponents of the disinformation campaign known as the “Health Freedom Movement” or the “Medical Freedom Movement”, which has since evolved into the “Make America Healthy Again” campaign, have invoked patriotism as justification for declaring freedom from vaccine mandates.32 Yet they overlook that fact that the patriots who fought in the American Revolutionary War were all variolated (a predecessor to vaccination in which individuals were exposed to small amounts of live virus to cause a mild case of the disease) against smallpox by order of General George Washington at Valley Forge during the winter of 1777-78. Historical records show that variolation reduced smallpox mortality from approximately 30% to less than 2%, a dramatic improvement in survival that enabled military operations to continue. A true patriot would recognize that vaccination against communicable diseases protects compatriots from preventable harm,33 readily agreeing to be vaccinated.
Another tactic of the anti-vaxxers is to challenge the science behind vaccines. Another irony, because the science that brought us vaccines is the same science that developed drugs to treat diabetes, heart, lung, kidney and many other diseases; radio, television, radar and global positioning systems (GPSs). How is it that we should only trust science when it has not been targeted by politicians who have an anti-science agenda when science conflicts with their policies? Remarkably, the scientific methods (i.e., hypothesis generation, experimental testing, peer review, and replication) have proven its validity across all fields. Selective rejection of science only when it conflicts with political agendas reveals motivated reasoning rather than legitimate scientific critique.
These anti-science, anti-vaccine activists have taken a page from the tobacco lobby’s strategy of hiring contrarian health professionals to dispute the evidence that smoking tobacco caused cancer, lung and heart disease. Put simply, their strategy was to create doubt to establish a controversy against the overwhelming scientific evidence that their products harmed people.34 Indeed, this strategy is also being used by the fossil fuel industry: “Should the public come to believe that the scientific issues are settled, their views about global warming will change accordingly. Therefore, you need to continue to make the lack of scientific certainty a primary issue in the debate.”35 For a more in depth discussion of the value reasonable doubt in science versus the cost of unreasonable doubt to science see: Allison et al.36
This strategy also creates a “false balance” whereby the arguments of a small number of contrarians who refute the scientific evidence are equated with the overwhelming majority of health professionals who are guided by the scientific evidence. The scientific consensus on vaccine safety and efficacy is comparable to that on climate change or evolution: based on thousands of peer-reviewed studies, systematic reviews, and decades of real-world data. Anti-vaccine activists also exploit the inherent uncertainty in science, arguing that incomplete knowledge invalidates all scientific data. This argument is logically fallacious. Science operates through progressive refinement of understanding, not absolute certainty. All empirical knowledge contains uncertainty, yet this does not negate its utility. Commercial aviation provides an apt analogy: while no flight can be guaranteed 100% crash-free, rigorous safety systems based on engineering principles and accident analysis have made air travel statistically the safest mode of transportation, with a fatality rate of approximately 0.07 per billion passenger miles.
Yet another misrepresentation of the anti-vaxxers is to claim that too many vaccines are being administered to infants such that they overwhelm their immune systems. The inaccuracy of this claim is described by Paul Offit in the book “Bad Advice”
“From the birth canal and beyond infants are confronted by a host of different challenges to the immune system.” (p 154)37
“The newborn has billions of immunological cells that are capable of responding to millions of different microorganisms.” “Therefore the combination of the three vaccines contained in MMR, or even the ten vaccines given in the first two years of life, is literally a raindrop in the ocean of what infants successfully encounter in their environment every day.” (p. 154)37
“Frankly, a scraped knee is a far greater immunological challenge than all of the childhood vaccines combined.” (p. 66)37
Notably, the greatest threat to the public health benefits of vaccination are the politicians who not only deny the evidence-based science supporting the safety and efficacy of vaccines, but who also appoint credentialed physicians and scientists to advocate against the principles upon which their credentials and training are based. The tension between public health practice and policy decisions is exemplified by recent changes in Florida's vaccination guidance under Surgeon General Joseph Ladapo, M.D., Ph.D., whose appointment and policy positions diverged from previous state public health recommendations. Previous state guidance had aligned with CDC recommendations regarding vaccination requirements, e.g. mandated vaccinations for children to attend school, and pandemic mitigation measures. The policy shift reflected broader debates during the COVID-19 pandemic regarding the balance between public health interventions and individual autonomy.
Ladapo had achieved some degree of notoriety as a member of “America’s Frontline Doctors” a group that was promoting the use of ivermectin and hydroxychloroquine as treatments for COVID-19 while downplaying the seriousness of the disease. The group also claimed to be a provider of legal services for people who refused to be vaccinated or have their children vaccinated, or refused to wear masks, receiving support from the “Tea Party Patriots” a Trump-aligned group.38
On his first day on the job, Ladapo challenged mask requirements to curb the spread of SARS-CoV-2 and signed an emergency rule that repealed required quarantines for schoolchildren who were exposed to COVID-19.39 Ladapo's public statements have included comparing vaccine mandates to historical injustices such as slavery, which appears as a characterization that public health ethicists note conflates voluntary medical interventions with involuntary servitude and may undermine discourse on both vaccination policy and historical human rights violations.40
In public health guidance regarding indoor air quality, recommendations have occasionally diverged from evidence-based best practices. For instance, suggestions to mitigate gas stove emissions through increased ventilation may not adequately address exposure in climate-controlled environments or areas with outdoor air quality concerns, where evidence indicates that alternative cooking methods provide more reliable risk reduction. Yet, in a 2023 speech to health professional students at Nova Southeastern University, Ladapo advocated for gas stoves in homes, despite acknowledging that they contribute to indoor air pollution which worsens asthma in children, recommending people should ‘just open the windows’ as a solution.
Concerns have been raised regarding possible trace DNA in mRNA vaccine preparations, with claims that such residual manufacturing components pose safety risks. However, regulatory analyses by the FDA and EMA determined that DNA quantities present in approved vaccines fall well below established safety thresholds and undergo rapid degradation in vivo, presenting negligible integration risk. These trace amounts are substantially lower than DNA exposures from dietary sources, environmental contact, or the human virome, which is approximately 8% of the human genome and consists of endogenous retroviral sequences integrated over evolutionary history. Yet updated guidance from the Ladapo directed Florida Department of health in 2024 opposed the use of COVID-19 booster vaccinations because they might contain small amounts of DNA.41 When vaccine risk communication incorporates theological or metaphysical frameworks (e.g., characterizing vaccines as "anti-Christ") a statement made by Ladapo during an interview on Steve Bannon’s “The War Room” on January 4, 2024, this departs from evidence-based public health discourse and may create barriers to informed medical decision-making. Recently, 12 former commissioners of the United States FDA warned of the threat to evidence-based vaccine policy and public health security arising from the proposed dramatic changes in vaccine advisory information disseminated by the FDA under the Trump administration.42
Ladapo has also advocated for the removal of fluoride from Florida’s drinking water,43 despite fluoridation of water to prevent tooth decay being touted as one of the greatest public health advances of the 20th century by the CDC.44 His misinterpretation of the effects of fluoridation of water are easily refuted by fact-based analyses of the substantial benefits and negligible risks of water fluoridation in the US.45-47 On May 13, 2025 Florida Governor Ron DeSantis signed a law effectively banning addition of fluoride to public water supplies.48
Most recently, Ladapo, in collaboration with another vaccine skeptic, Retsev Levi from the MIT School of Management, published a manuscript on the preprint server medRxiv49 that uses the technique of distraction to denigrate mRNA vaccines. Titled “Twelve- Month All-Cause Mortality after Initial COVID-19 Vaccination with Pfizer-BioNTech or mRNA-1273 among Adults Living in Florida”, the manuscript describes a small difference in death rates between the two mRNA vaccines in matched cohorts. It then goes on to infer that the difference in death rates is due to unspecified off-target adverse reactions to the Pfizer-BioNTech vaccine compared to the Moderna mRNA-1273 vaccine. Of note, data from only 16% of the population of Floridians who received the two vaccines were reported in the main text of the manuscript. Surprisingly, a supplementary figure in the manuscript (Supplementary Figure 3), not described in the main text, revealed an opposite finding: all cause deaths, cardiovascular disease deaths, and non-COVID-19 deaths were all greater following the Moderna mRNA-1273 vaccine, while only COVID-19 deaths were higher with the Pfizer-BioNTech vaccine, suggesting that the Moderna vaccine simply gave better protection against the evolving variants (especially the delta variant) of SARS-CoV-2. A critical methodological limitation was the absence of an unvaccinated comparison group, which prevents assessment of whether observed mortality differences reflected vaccine effects or baseline population characteristics. This analytical approach, presenting relative comparisons between two vaccine types without an unvaccinated reference group, limits causal inference.50 Similar concerns regarding data completeness and analysis methodology have been raised about previous Florida Department of Health reports on vaccine safety, where independent researchers noted that age-stratified analyses presented in public guidance omitted broader age-group data that showed different risk patterns. Such selective reporting practices raise ethical concerns about data transparency and the reproducibility of safety analyses used to inform public health policy, specifically with respect to the claim that mRNA vaccines increased cardiac-related deaths in 18-29-year-old men.51
An argument trumpeted by Ladapo and other anti-vaccine activists is that vaccination against communicable diseases is a matter of personal choice, insisting that individuals should be allowed to “do their own research”. While personal autonomy is, in principle, a right that should be afforded to individuals, it becomes compromised when the information landscape is flooded with misinformation. When politically motivated disinformation drowns out accurate scientific content, people can be easily misled into making choices that endanger their own health and the health of others. To analogize, it is as if most of the information available to drivers claimed that driving drunk is harmless, and a personal choice, leading them to drive while intoxicated.
Addressing vaccine hesitancy requires distinguishing between legitimate scientific uncertainty, which is inherent to all empirical research, and systematic misrepresentation of evidence. When public health policy departs from established scientific consensus without corresponding advances in evidence, this creates challenges for both clinical practice and public trust. Strengthening the interface between research evidence and health policy may require enhanced transparency in how scientific data inform policy decisions, clearer communication of the evidentiary basis for recommendations, and mechanisms to ensure that policy positions remain responsive to the evolving scientific literature.
On September 3, 2025 Florida Surgeon General Ladapo announced that the State of Florida would now push to scrap all vaccine and immunization requirements — most notably including those for students entering schools, making Florida the first state to abandon vaccine mandates for communicable diseases.52
Perhaps by exposing the unethical practices of those who dispute vaccines for reprehensible political purposes, we can reverse the degeneration of public health policy by those who maliciously and falsely argue against vaccine safety and efficacy. However, we need to go beyond the domain of the scientific community and reach out to the public, either by community outreach, media interviews, letters to editors and Op-Eds that convey the value of vaccination, thereby opposing the anti-science, anti-vaccination disinformation campaigns. We need to translate our scientific jargon into language that the public can understand so that they can make informed decisions about vaccination based upon the best available science.
Remarkably, vaccine-hesitant individuals often exhibited distorted benefit-risk calculations. Measles vaccination can reduce the incidence of measles-induced encephalitis in unvaccinated infected children (approximately 1 per 1,000), to rates below 1 per 1,000,000 vaccine doses -- a thousandfold safety margin. However, psychological research demonstrates that individuals weigh potential harms from intervention (commission bias) more heavily than equivalent harms from inaction (omission bias). Parents report greater regret anticipation of their child experiencing a vaccine adverse event versus contracting a vaccine-preventable disease, even when the latter carries substantially higher morbidity risk. Perceived barriers extend beyond medical concerns to include logistical factors (appointment scheduling, cost, access), misinformation exposure, together with possible distrust of pharmaceutical companies or government recommendations. The Wakefield fraud's enduring impact exemplifies how a single fraudulent study can erect persistent psychological barriers that rigorous contradictory evidence struggles to dismantle —a phenomenon termed "continued influence effect" in cognitive psychology.53-56
Of note, vaccine safety in the United States is monitored through a comprehensive three-tiered surveillance systems, including the VAERS, VSD, and CISA Project, that enables continuous surveillance of millions of vaccinations annually, providing robust data on safety profiles. This multi-layered approach, combining passive reporting, active population-level surveillance, and detailed clinical assessment, ensures that vaccine safety is continuously monitored with scientific rigor, allowing public health officials to detect even rare adverse events and make evidence-based recommendations to protect public health. Altogether, the risk-benefit analysis for vaccines overwhelmingly favors vaccination. As a result, while deciphering all aspects of immunity, precision vaccination modalities will remain one of the most effective means to control emerging/reemerging infectious diseases.
Competing Interests
The author has no conflicts of interests that pertain to this commentary.
Ethical Approval
Not applicable.
Acknowledgements
The author thanks Dr. Lisa S. Robison for her review and editorial recommendations for improvement of this manuscript.
References
- Plotkin SL, Plotkin SA. A short history of vaccination. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 1-16.e9. doi: 10.1016/b978-0-323-79058-1.00001-3.
- Nussbaum L, Schwab J, Tayman A, Thombley M, Watts L. Legal issues. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 1704-37.e6. doi: 10.1016/b978-0-323-79058-1.00085-2.
- Douglas RG, Samant VB. The vaccine industry. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 52-63. doi: 10.1016/b978-0-323-79058-1.00005-0.
- Marshall VB, Gruber MF. Regulation and testing of vaccines in the US. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 1640-59.e2. doi: 10.1016/b978-0-323-79058-1.00080-3.
-
DeStefano F, Fisher AM, Shimabukuro TT, Offit PA. Vaccine safety. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 1679-95.e10. doi: 10.1016/b978-0-323-79058-1.00083-9.
- Center for Biologics Evaluation and Research (CBER). Development and Licensure of Vaccines to Prevent COVID-19: Guidance for Industry. CBER; 2023. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/development-and-licensure-vaccines-prevent-covid-19.
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med 2020; 383:2603-15. doi: 10.1056/NEJMoa2034577 [Crossref] [ Google Scholar]
-
Perlman S, Denison MR. Coronavirus vaccines. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 248-57.e9. doi: 10.1016/b978-0-323-79058-1.00017-7.
- Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med 2021; 384:403-16. doi: 10.1056/NEJMoa2035389 [Crossref] [ Google Scholar]
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N Engl J Med 2020; 383:2603-15. doi: 10.1056/NEJMoa2034577 [Crossref] [ Google Scholar]
- Haber P, Parashar UD, Haber M, DeStefano F. Intussusception after monovalent rotavirus vaccine-United States, Vaccine Adverse Event Reporting System (VAERS), 2008-2014. Vaccine 2015; 33:4873-7. doi: 10.1016/j.vaccine.2015.07.054 [Crossref] [ Google Scholar]
-
Robinson JM, Gomez Iii PL, Rogalewicz JA, Havelange N, Sitrin RD, Gervier R. Vaccine manufacturing. In: Orenstein W, Offit P, Edwards KM, Plotkin S, eds. Plotkin's Vaccines. 8th ed. Philadelphia: Elsevier; 2023. p. 64-76. doi: 10.1016/b978-0-323-79058-1.00006-2.
- Weber L, Clement S, Guskin E, Sun LH. Why 1 in 6 U.S. Parents Are Rejecting Vaccine Recommendations. The Washington Post; 2025. Available from: https://www.washingtonpost.com/health/2025/09/15/childhood-vaccines-parents-post-kff-poll/.
- Stuart JF. £30,000 for the Cow-Pox!!! An Address (to Ld. H.P., and) to the British Parliament, on Vaccination; (of the Greatest Importance to Mankind) Wherein the Report of the College of Physicians is Completely Confuted. London: London School of Hygiene and Tropical Medicine; 1807. Available from: https://wellcomecollection.org/works/uxzrhbty.
- Barzegari A, Saeedi N, Zarredar H, Barar J, Omidi Y. The search for a promising cell factory system for production of edible vaccine. Hum Vaccin Immunother 2014; 10:2497-502. doi: 10.4161/hv.29032 [Crossref] [ Google Scholar]
- Omidi Y, Pourseif MM, Ansari RA, Barar J. Design and development of mRNA and self-amplifying mRNA vaccine nanoformulations. Nanomedicine (Lond) 2024; 19:2699-725. doi: 10.1080/17435889.2024.2419815 [Crossref] [ Google Scholar]
- Parvizpour S, Pourseif MM, Razmara J, Rafi MA, Omidi Y. Epitope-based vaccine design: a comprehensive overview of bioinformatics approaches. Drug Discov Today 2020; 25:1034-42. doi: 10.1016/j.drudis.2020.03.006 [Crossref] [ Google Scholar]
- Parvizpour S, Razmara J, Pourseif MM, Omidi Y. In silico design of a triple-negative breast cancer vaccine by targeting cancer testis antigens. Bioimpacts 2019; 9:45-56. doi: 10.15171/bi.2019.06 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Daghighkia H, Nematollahi A, Omidi Y. A novel B- and helper T-cell epitopes-based prophylactic vaccine against Echinococcus granulosus. Bioimpacts 2018; 8:39-52. doi: 10.15171/bi.2018.06 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Naghili B, Saeedi N, Parvizpour S, Nematollahi A. A novel in silico minigene vaccine based on CD4 + T-helper and B-cell epitopes of EG95 isolates for vaccination against cystic echinococcosis. Comput Biol Chem 2018; 72:150-63. doi: 10.1016/j.compbiolchem.2017.11.008 [Crossref] [ Google Scholar]
- Pourseif MM, Moghaddam G, Saeedi N, Barzegari A, Dehghani J, Omidi Y. Current status and future prospective of vaccine development against Echinococcus granulosus. Biologicals 2018; 51:1-11. doi: 10.1016/j.biologicals.2017.10.003 [Crossref] [ Google Scholar]
- Pourseif MM, Parvizpour S, Jafari B, Dehghani J, Naghili B, Omidi Y. A domain-based vaccine construct against SARS-CoV-2, the causative agent of COVID-19 pandemic: development of self-amplifying mRNA and peptide vaccines. Bioimpacts 2021; 11:65-84. doi: 10.34172/bi.2021.11 [Crossref] [ Google Scholar]
- Safary A, Akbarzadeh-Khiavi M, Barar J, Omidi Y. SARS-CoV-2 vaccine-triggered autoimmunity: molecular mimicry and/or bystander activation of the immune system. Bioimpacts 2023; 13:269-73. doi: 10.34172/bi.2023.27494 [Crossref] [ Google Scholar]
- Salemi A, Pourseif MM, Masoudi-Sobhanzadeh Y, Ansari R, Omidi Y. Proteome-wide reverse vaccinology to identify potential vaccine candidates against Staphylococcus aureus. Mol Immunol 2025; 183:296-312. doi: 10.1016/j.molimm.2025.05.016 [Crossref] [ Google Scholar]
-
Retraction--Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Lancet 2010; 375: 445. doi: 10.1016/s0140-6736(10)60175-4.
- Deer B. Secrets of the MMR scare How the vaccine crisis was meant to make money. BMJ 2011; 342:c5258. doi: 10.1136/bmj.c5258 [Crossref] [ Google Scholar]
- Deer B. How the case against the MMR vaccine was fixed. BMJ 2011; 342:c5347. doi: 10.1136/bmj.c5347 [Crossref] [ Google Scholar]
- DeStefano F, Shimabukuro TT. The MMR vaccine and autism. Annu Rev Virol 2019; 6:585-600. doi: 10.1146/annurev-virology-092818-015515 [Crossref] [ Google Scholar]
- Hviid A, Hansen JV, Frisch M, Melbye M. Measles, mumps, rubella vaccination and autism: a nationwide cohort study. Ann Intern Med 2019; 170:513-20. doi: 10.7326/m18-2101 [Crossref] [ Google Scholar]
- Taylor LE, Swerdfeger AL, Eslick GD. Vaccines are not associated with autism: an evidence-based meta-analysis of case-control and cohort studies. Vaccine 2014; 32:3623-9. doi: 10.1016/j.vaccine.2014.04.085 [Crossref] [ Google Scholar]
- Anthes E, Rosenbluth T. Vaccine Skepticism Comes for Pet Owners, Too. The New York Times; 2025. Available from: https://www.nytimes.com/2025/10/27/science/vaccines-pets-dogs-cats.html.
- Zimmerman A. Patriotism, Rights, and Vaccination. Bioethics Today; 2021.
- Fenn EA. Biological warfare in eighteenth-century North America: beyond Jeffery Amherst. J Am Hist 2000; 86:1552-80. [ Google Scholar]
- Michaels D. Doubt is Their Product: How Industry's Assault on Science Threatens Your Health. Oxford University Press; 2008.
- Conway-Wood S. “Doubt is Our Product” – The Dark Marketing Tactics Big Oil Took Straight from the Big Tobacco Playbook. Ethical Hour Ltd; 2022. Available from: https://ethicalhour.com/in-house/reshare/doubt-is-our-product-the-dark-marketing-tactics-big-oil-took-straight-from-the-big-tobacco-playbook/.
- Allison DB, Pavela G, Oransky I. Reasonable versus unreasonable doubt: although critiques of scientific findings can be used for misleading purposes, skepticism still plays a crucial role in producing robust research. Am Sci 2018; 106:84-8. doi: 10.1511/2018.106.2.84 [Crossref] [ Google Scholar]
- Offit P. Bad Advice: Or Why Celebrities, Politicians, and Activists Aren't Your Best Source of Health Information. New York: Columbia University Press; 2018.
- Bergengruen V. How ‘America’s Frontline Doctors’ Sold Access to Bogus COVID-19 Treatments—and Left Patients in the Lurch. Time Magazine; 2021. Available from: https://time.com/6092368/americas-frontline-doctors-covid-19-misinformation/.
- Sarkissian A. How a Doctor Who Questioned Vaccine Safety Became Desantis’ Surgeon General Pick. Politico; 2021. Available from: https://www.politico.com/news/2021/10/07/how-a-doctor-who-questioned-vaccine-safety-became-desantis-surgeon-general-pick-515574.
- Epstein K. The Florida Surgeon General Who Likens Vaccine Mandates to Slavery. BBC; 2025. Available from: https://www.bbc.com/news/articles/c62q41qm9pvo.
- Florida Department of Health. Updated Guidance for COVID-19 Boosters for the Fall and Winter 2024-2025 Season. Florida Department of Health; 2025. Available from: https://www.floridahealth.gov/newsroom/2024/09/20210912-UpdatedGuidanceCOVID-19.html.
-
Califf RM, von Eschenbach AC, Friedman MA, Giroir BP, Gottlieb S, Hamburg MA, et al. A threat to evidence-based vaccine policy and public health security at the FDA. N Engl J Med 2025. doi: 10.1056/NEJMp2517497.
- Florida Department of Health. State Surgeon General Dr. Joseph A. Ladapo Issues Community Water Fluoridation Guidance. Florida Department of Health; 2024. Available from: https://www.floridahealth.gov/newsroom/2024/11/20241122-fluoridation-guidance.pr.html.
- Centers for Disease Control and Prevention (CDC). About Community Water Fluoridation. CDC; 2024. Available from: https://www.cdc.gov/fluoridation/about/index.html#%3A~%3Atext%3DCDC%20named%20fluoridation%20of%20drinking%2Cwater%20fluoridation%20started%20in%201945.
- Levy SM. Caution needed in interpreting the evidence base on fluoride and IQ. JAMA Pediatr 2025; 179:231-4. doi: 10.1001/jamapediatrics.2024.5539 [Crossref] [ Google Scholar]
-
Speth RC. Concerns about data and analyses used in assessing fluoride exposure and children's IQ scores. JAMA Pediatr 2025. doi: 10.1001/jamapediatrics.2025.0929.
- Warren JR, Rumore G, Kim S, Grodsky E, Muller C, Manly JJ. Childhood fluoride exposure and cognition across the life course. Sci Adv 2025; 11:eadz0757. doi: 10.1126/sciadv.adz0757 [Crossref] [ Google Scholar]
- Cochrane E. Florida Just Banned Fluoride from Public Water. Here’s What to Know. The New York Times; 2025. Available from: https://www.nytimes.com/2025/05/15/us/politics/florida-fluoride-water-ban.html.
- Levi R, Mansuri F, Jordan MM, Ladapo JA. Twelve-Month All-Cause Mortality after Initial COVID-19 Vaccination with Pfizer-BioNTech or mRNA-1273 among Adults Living in Florida. medRxiv [Preprint]. April 29, 2025. Available from: https://www.medrxiv.org/content/10.1101/2025.04.25.25326460v1.
- Florida Department of Health. State Surgeon General Dr. Joseph A. Ladapo Issues New MRNA COVID-19 Vaccine Guidance. Florida Department of Health; 2022. Available from: https://www.floridahealth.gov/_documents/newsroom/press-releases/2022/10/20221007-guidance-mrna-covid19-vaccines.pr.pdf.
- Lemongello S, Catherman C. Ladapo’s Escalating Vaccine War is a DeSantis Campaign Strategy, Critics Argue. Orlando Sentinel; 2024. Available from: https://www.orlandosentinel.com/2024/01/13/ladapos-escalating-vaccine-war-is-a-desantis-campaign-strategy-critics-argue/.
- Hibbert CM. Florida’s Plan to Phase Out Childhood Vaccination Mandates Upends Decades of Public Health Policy, Northeastern Experts Say. Northeastern Global News; 2025. Available from: https://news.northeastern.edu/2025/09/05/florida-vaccine-mandates-ending/#:~:text=University%20News-,Floridas%20plan%20to%20phase%20out%20childhood%20vaccination%20mandates%20upends%20decades,vaccination%20requirements%20for%20school%20attendance.
- Pluviano S, Watt C, Della Sala S. Misinformation lingers in memory: failure of three pro-vaccination strategies. PLoS One 2017; 12:e0181640. doi: 10.1371/journal.pone.0181640 [Crossref] [ Google Scholar]
- Connolly T, Reb J. Omission bias in vaccination decisions: where’s the “omission”? Where’s the “bias”?. Organ Behav Hum Decis Process 2003; 91:186-202. doi: 10.1016/s0749-5978(03)00057-8 [Crossref] [ Google Scholar]
- Ritov I, Baron J. Reluctance to vaccinate: omission bias and ambiguity. J Behav Decis Mak 1990. 3: 263-77. doi: 10.1002/bdm.3960030404.
- Pardi N, Hogan MJ, Porter FW, Weissman D. mRNA vaccines - a new era in vaccinology. Nat Rev Drug Discov 2018; 17:261-79. doi: 10.1038/nrd.2017.243 [Crossref] [ Google Scholar]