Bioimpacts. 16:31081.
doi: 10.34172/bi.31081
Review
The emergence of advanced technologies in the pharmacy profession and the need for education: The case of point-of-care sensing systems and 3D printing of pharmaceuticals
Jaleh Barar Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, 1 
Matthew Seamon Validation, Writing – review & editing, 2
Yadollah Omidi Conceptualization, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing, 1, *
Author information:
1Department of Pharmaceutical Sciences, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
2Department of Pharmacy Practice, Barry and Judy Silverman College of Pharmacy, Nova Southeastern University, Fort Lauderdale, FL 33328, USA
Abstract
Introduction:
The pharmacy profession is undergoing significant transformation through the adoption of point-of-care testing (POCT) and three-dimensional (3D) printing of pharmaceuticals. These technologies offer enhanced diagnostic accuracy, faster therapeutic interventions, and the potential for personalized medication regimens. Accordingly, there lies a great need for proper education.
Methods:
A comprehensive literature review was conducted to explore the impacts and current educational integration of POCT and 3D printing of pharmaceuticals in the pharmacy profession, and a qualitative analysis was performed.
Results:
Through the integration of POCT into community and clinical settings, pharmacists can promptly identify health conditions and provide timely referrals or interventions, ultimately improving patient outcomes. Additionally, 3D printing allows for the creation of highly customized dosage forms, supporting targeted drug delivery and better patient adherence. These innovations necessitate adjustments in pharmacy education to equip future professionals with the requisite clinical and technical skills to provide value to the healthcare system. Pharmacy educators must be current in their knowledge. Curricula must emphasize hands-on experiences, such as simulations and laboratory training, to foster proficiency in using diagnostic devices, interpreting results, and designing bespoke drug formulations. Interprofessional collaboration, policy development, advocacy, and ongoing faculty training are also crucial for ensuring that pharmacists remain at the forefront of technological advancements. This context underscores the importance of weaving these modern tools into educational strategies.
Conclusion:
By preparing pharmacists for expanded and more technical roles in healthcare, including diagnostics and medication customization, schools and colleges of pharmacy can propel the profession forward and elevate the standard of patient care in rapidly evolving healthcare environments and improve patient outcomes, thereby providing critical cost savings to the system.
Graphical Abstract
Keywords: 3D printing, Curriculum innovation, Healthcare transformation, Personalized precision medicine, Pharmacy profession, Point-of-care testing
Copyright and License Information
© 2026 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
None to be declared.
Introduction
Pharmacy education is nascent in response to technological advancements and the expanding role of pharmacists in healthcare.1 From point-of-care testing (POCT) and sensing systems to novel manufacturing processes such as three-dimensional (3D) printing, these innovations present both opportunities and challenges for pharmacy curricula and professional practice. A growing body of literature underscores the need to integrate new technologies into pharmacy education to meet the changing demands of patient care and prepare future pharmacists for increasingly complex clinical roles.2,3 This paper provides an overview of how POCT has become integral to pharmacy practice, highlights the potential for 3D printing in pharmaceutical education, and discusses the implications for curriculum design and professional development.
Pharmacy practice has traditionally focused on dispensing medications and providing patient counseling. However, in recent years, there has been a marked shift toward more patient-centric and clinically oriented services involving medication optimization and safety.4 This shift includes administering immunizations, managing chronic diseases, and conducting medication therapy management (MTM) programs.
More recently, pharmacists have begun to adopt POCT services, especially in community settings, to improve patient access to diagnostic testing and improve clinical outcomes.5 These broader responsibilities require corresponding enhancements in pharmacy education so that future pharmacists are equipped with the necessary skills to interpret clinical data and deliver evidence-based interventions.6
Meanwhile, 3D printing (the so-called additive manufacturing), which involves layer-by-layer fabrication of objects from digital models, holds promise for precision and personalized medicine in this patient-centric model.
This forces a necessary revision in the pharmacy curriculum to meet the needs of such precision bioengineered medicines and advances in patient care. For example, bio-GMP laboratories, similar to drug formulation, will be essential for the bioformulation of cell- and/or tissue-based medicines and available to student learners. This review aims to highlight the importance of the integration of emerging technologies in the current pharmacy curriculum for training pharmacists with such expertise. Table 1 summarizes the influence of different disciplines relevant to futuristic pharmacy, the key competencies/skills, and potential impact/applications.
Table 1.
The impacts of different disciplines, key skills, and applications in the transformation of pharmacy profession
|
Field
|
Relevance to futuristic pharmacy
|
Key competencies and skills
|
Potential impact and applications
|
Ref.
|
| Point-of-care testing (POCT) |
Enables rapid, on-site diagnostic insights, facilitating immediate therapeutic interventions in community and clinical settings |
- Proficiency in operating and maintaining POCT devices
- Ability to interpret and act upon test results
- Knowledge of relevant clinical guidelines and patient counseling |
- Early disease detection and rapid intervention
- Improved patient follow-up and adherence
- Reduced burden on secondary healthcare facilities |
2,7
|
| 3D printing |
Facilitates the creation of customized dosage forms, allowing for targeted drug delivery, improved medication adherence, and adaptation to individual patient needs |
- Understanding of 3D printing processes and materials
- Skills in designing dosage forms and adjusting drug release profiles
- Awareness of regulatory and quality standards |
- Personalized medication regimens
- Enhanced patient compliance through customized forms
- Development of specialized implants and devices |
8-10
|
| Personalized formulations |
Supports patient-specific therapies through tailored drug concentrations, release profiles, and innovative materials (e.g., bioinks) |
- Competence in pharmaceutical compounding and formulation design
- Knowledge of pharmacokinetics, pharmacodynamics, and biomaterials
- Familiarity with bioinks and novel excipients |
- Precision medicine with optimized therapeutic outcomes
- Reduced adverse effects via dose individualization
- Possibility of on-demand manufacturing for rare or orphan conditions |
11
|
| Clinical and technical skills |
Integral for handling advanced diagnostic tools, interpreting complex data, and performing specialized procedures in rapidly evolving healthcare settings |
- Clinical decision-making and problem-solving
- Mastery of advanced laboratory techniques (e.g., molecular diagnostics)
- Technical troubleshooting of devices |
- Higher accuracy in medication therapy management
- Swift adjustment of treatment plans based on diagnostic data
- Increased trust and collaboration with other healthcare professionals |
- |
| Interprofessional collaboration |
Ensures seamless integration of pharmacists’ roles with physicians, nurses, and other healthcare professionals for comprehensive patient care |
- Strong communication and team-building skills |
- Improved patient outcomes through coordinated care |
|
- Cross-disciplinary understanding of healthcare workflows
- Ability to coordinate care and collaborate on complex patient cases |
- Enhanced workflow efficiency in clinical settings
- Shared responsibility in designing and evaluating treatment regimens |
- |
| Policy and regulatory affairs |
Governs ethical deployment of novel technologies like POCT and 3D printing in pharmacy practice, including licensure, scope of practice, and quality assurance |
- Knowledge of healthcare policies and regulations
- Familiarity with intellectual property and device certification processes
- Advocacy skills for shaping practice standards |
- Compliance with local and global regulations
- Protection of patient safety and privacy
- Facilitation of swift technology adoption and standardization
- Pharmaceutical industry |
12-14
|
| Faculty training and education |
Essential for updating curricula to include hands-on experiences with emerging technologies, ensuring that upcoming pharmacy professionals are well-prepared |
- Curriculum development and instructional design
- Technological proficiency (3D printers, POCT devices)
- Continuous professional development and research integration |
- Production of highly skilled pharmacy graduates
- Ongoing innovation in teaching methods
- Stronger research collaborations and industry partnerships |
15-18
|
| Data analytics and digital health |
Critical for analyzing large sets of patient data from POCT devices and 3D-printed medication outcomes, leading to evidence-based decisions and optimized patient care |
- Competence in data interpretation and statistical analysis
- Familiarity with electronic health record systems
- Ability to safeguard patient data (cybersecurity and privacy) |
- Personalized, data-driven interventions
- Enhanced tracking of patient outcomes for continuous improvement
- Innovation in remote and telehealth pharmacy services |
19-21
|
Emerging technologies in pharmacy education and profession
Emerging technologies are rapidly reshaping pharmacy practice, pushing the profession beyond traditional dispensing toward data-driven, patient-centered, and personalized care. This raises the need for pharmacy students to be competent practitioners in these fields. Specifically, POCT can provide real-time clinical insights, while in-pharmacy 3D printers enable on-demand production of customized dosage forms that match individual pharmacogenomic profiles or dynamic therapeutic needs. Artificial intelligence augments these capabilities by predicting adherence risks, optimizing inventory, and guiding precision dosing algorithms. Simulated reality platforms (as virtual, augmented, and mixed approaches) provide immersive skills training that replicates complex clinical scenarios without risking patient safety. Further, blockchain-anchored supply chains bolster drug authenticity and traceability.22 Collectively, these tools demand new curricular content in coding, quality-by-design, data analytics, and human-factor engineering, preparing graduates to navigate a healthcare landscape where the pharmacist acts simultaneously as diagnostician, formulator, and informatics specialist. Fig. 1 represents schematic illustrations for emerging technologies in pharmacy education and profession.
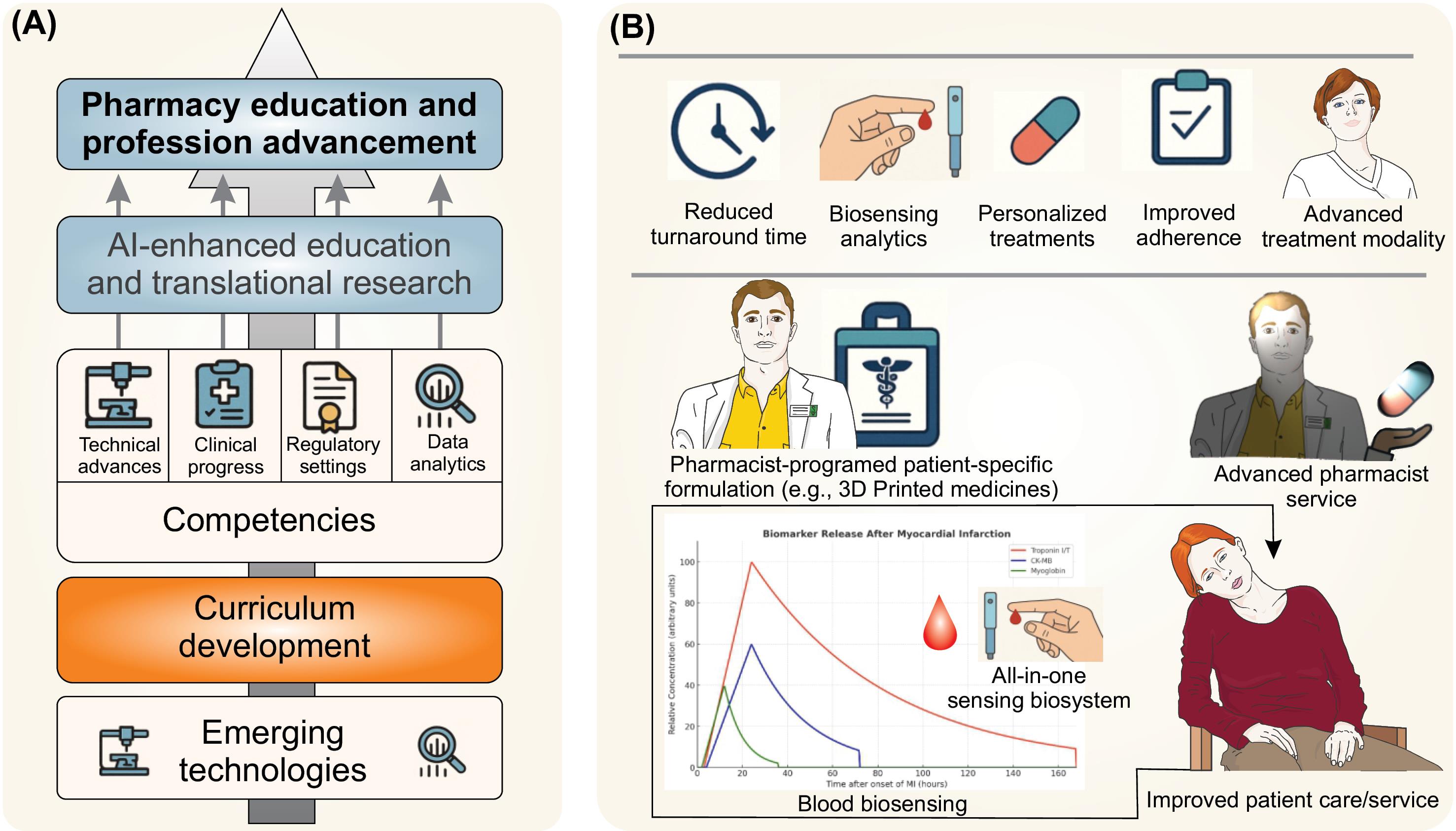
Fig. 1.
Emerging technologies in pharmacy education and profession. A) Integration of emerging technologies and their competencies in pharmacy education and profession. B) The impacts of POCT and 3D printing of medications.
.
Emerging technologies in pharmacy education and profession. A) Integration of emerging technologies and their competencies in pharmacy education and profession. B) The impacts of POCT and 3D printing of medications.
Potential benefits and applications of POCT and 3D Printing
The principal advantage of integrating 3D printing into pharmacy education lies in its capacity to deepen students’ understanding of pharmaceutical compounding, drug formulation, and personalized medicine. By allowing precise control over drug release profiles, shapes, and dosages, 3D printing can help illustrate the theoretical underpinnings of pharmaceutics in a tangible manner. Additionally, 3D-printed models or devices can serve as valuable educational aids, enabling students to visualize complex anatomical structures or drug delivery mechanisms more effectively than traditional diagrams or static models.
The technology also opens avenues for innovative patient-centered care. Students exposed to 3D printing processes gain firsthand experience in customizing therapy for specific patient needs. For instance, a patient who struggles with traditional pill-swallowing might benefit from a rapidly dissolving 3D-printed oral film with an individualized dose. Pharmacy education that incorporates such experiential learning can pave the way for new roles in advanced practice settings, strengthening the pharmacist’s position as a healthcare innovator. Fig. 2 represents the integration benefits of POCT and 3D printing in the pharmacy profession.
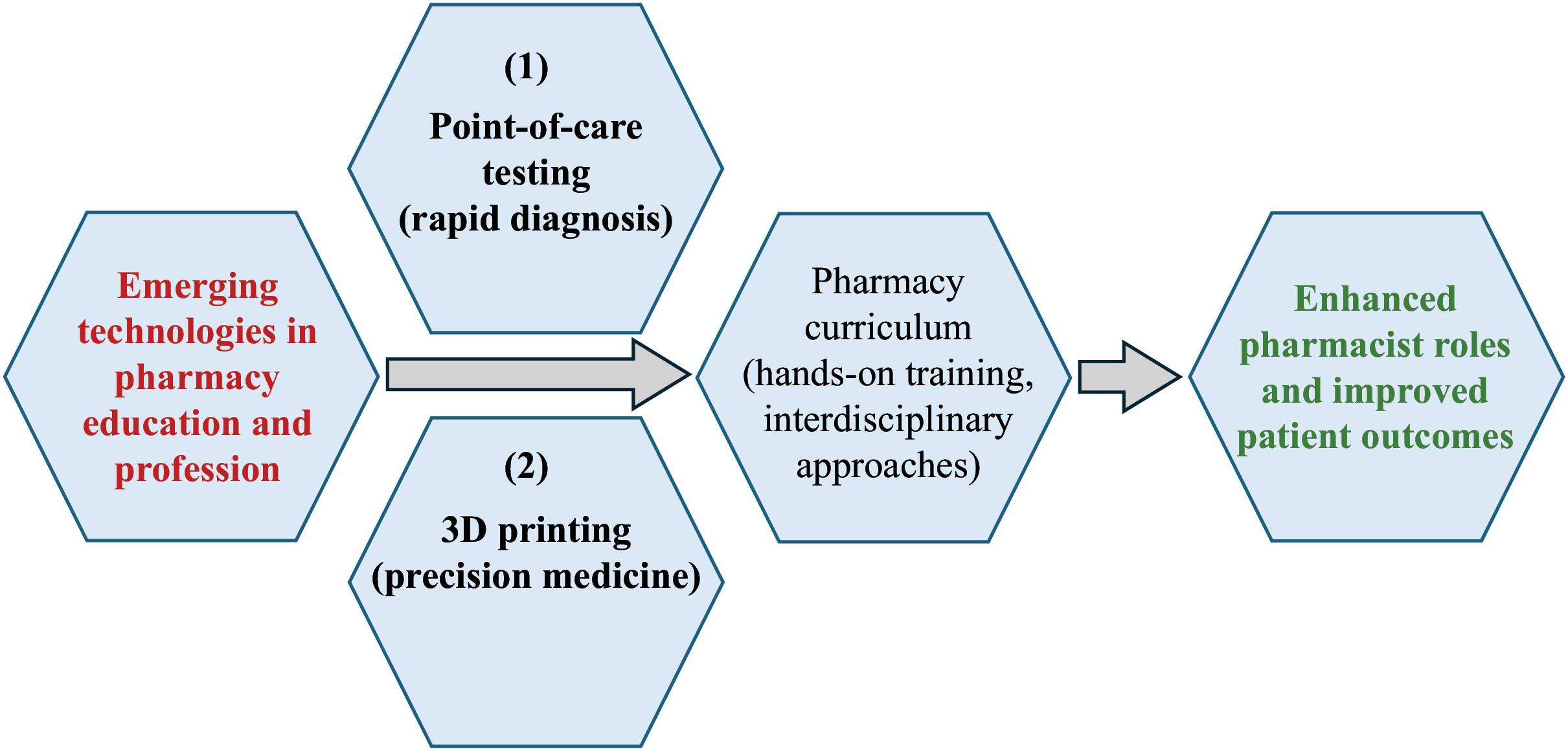
Fig. 2.
The integration benefits of POCT and 3D printing in the pharmacy profession.
.
The integration benefits of POCT and 3D printing in the pharmacy profession.
Diagnostic transformation via POCT
Point-of-care sensor system testing has recast the pharmacist’s role from passive dispenser to active clinician by shrinking the temporal and spatial gaps between specimen collection, result interpretation, and therapeutic decision-making. Modern handheld analyzers quantify biomarkers such as HbA1c, C-reactive protein, Influenza A, Streptococcus, and SARS-CoV-2 antigens within minutes, empowering pharmacists to initiate therapy during the same encounter, sometimes under a physician collaborative practice agreement or protocol. The immediate feedback not only accelerates disease management, reducing downstream transmission, hospital visits, and associated costs, but also strengthens patient engagement, as individuals receive real-time counseling while results are still top-of-mind. In underserved or rural settings, POCT further narrows health-equity gaps by providing greater access and bypassing wait times at centralized laboratories.1,23 Collectively, these advances reposition the pharmacy counter as a frontline diagnostic hub that supports chronic-disease monitoring, antimicrobial stewardship, and public-health surveillance.
Point-of-care testing and biosensing systems, state of the science, developing practicalities, and their educational value in pharmacy education
POCT refers to diagnostic tests that are performed near the site of patient care, offering rapid results that can guide clinical decision-making.1 Numerous studies have demonstrated the effectiveness of such tests when integrated into pharmacy practice. For instance, Sun et al proposed affordable colorimetric approaches for the on-site detection of metal ions,3 while Zhang et al designed a miniaturized colorimetric-photoacoustic device capable of detecting ascorbic acid in food.24 Although these studies primarily address diagnostic processes in broader contexts, they illustrate the portability and speed inherent in POCT systems—characteristics that have direct applicability in a pharmacy setting.
Pharmacy curricula that incorporate POCT often include hands-on laboratory workshops, simulations, and interprofessional education.6 From an educational standpoint, exposing student pharmacists to POCT has several benefits. First, practical involvement with POCT technologies fosters clinical reasoning with emerging technologies, as students must understand not only how to perform a test but also how to interpret results accurately. Second, POCT training equips students to navigate various clinical scenarios that require immediate therapeutic interventions, such as managing potential infections.23 Third, it introduces students to collaborative healthcare, whereby pharmacists coordinate with other professionals (e.g., physicians and nurses) and guide patients effectively based on on-site test findings.25
Kherghehpoush and McKeirnan highlight how community pharmacy-based screening for HIV and hepatitis C can broaden students’ understanding of infectious disease management while also refining their communication and counseling skills.26 The success of such programs suggests that incorporating clinical skill training with POCT in the education of future pharmacists can substantially enhance professional readiness and patient care outcomes.27 Further, pharmacy education is increasingly integrating innovative diagnostic technologies into its curricula, particularly POCT, and biosensors that enable rapid, accurate, and minimally invasive testing. These biosensors, which include electrochemical and optical platforms, are revolutionizing how pharmacists learn about disease diagnosis, therapeutic monitoring, and personalized treatment strategies.28 Their high specificity, sensitivity, and speed make them essential for early detection of critical biomarkers in a variety of diseases, such as cancer and kidney disorders.29,30
In the context of oncology, research has showcased immunosensors tailored to detect biomarkers like carcinoembryonic antigen and CA 15-3 for detection of cancers, including colon, breast, and lung.31,32 By offering ultra-low limits of detection, these devices give future pharmacists a practical illustration of how early disease diagnosis can be translated from bench to bedside. Modern biosensors, especially electrochemical immunosensors, exemplify how nanotechnology and biorecognition elements converge to enable rapid, ultrasensitive detection of disease biomarkers. For instance, sandwich-style immunosensors enhanced by nanoparticles can detect carcinoembryonic antigen (CEA) at concentrations as low as 58 fg/mL, demonstrating unprecedented specificity and sensitivity.28 Similarly, point-of-care detection of key cancer biomarkers, such as CA 15-3 and CA-125, has been achieved using electrochemical platforms with detection limits of 15 × 10⁻⁶ U/mL and 0.0016 U/mL, respectively.29,32 The capacity of these biosensors to detect minuscule amounts of markers enhances early diagnosis, subsequently improving therapeutic outcomes and overall patient survival rates. From a nephrology perspective, early detection of kidney dysfunction is vital to prevent disease progression,30 including biosensors that measure cystatin C levels offer a promising avenue for rapid and precise assessment of renal function, enabling pharmacists to guide appropriate interventions in a timely manner. Moreover, immunosensors designed for metabolic pathway assessment, such as the tryptophan-kynurenine pathway, reveal cancer cell immune evasion mechanisms and thereby support individualized immunotherapy decisions.33 Incorporating these advancements into pharmacy education fosters a workforce adept at harnessing point-of-care diagnostics. Trainees not only learn to interpret data from biosensors but also to communicate these findings to multidisciplinary teams and patients. By mastering biosensor technologies, graduates are empowered to improve medication therapy management, expedite diagnostic testing, and optimize patient-centric care in various clinical and community settings. As such, the integration of cutting-edge biosensor methodologies and POCT within pharmacy education is instrumental in shaping the next generation of pharmacists to be key contributors to precision medicine and public health.
Personalized drug formulation by 3D printing: state of the science, developing practicalities, and their educational value
Additive manufacturing brings precision pharmaceutics to the community level by allowing dose, geometry, and release profile to be customized on demand. Powder-bed and semisolid-extrusion printers now yield highly porous printlets that dissolve rapidly for dysphagic patients, multilayer tablets combining incompatible APIs, and pediatric chewables calibrated in one-tenth-milligram increments. Layer-by-layer fabrication also facilitates complex internal lattice structures, enabling zero-order or pulsatile release kinetics that were previously achievable only in industrial settings. When linked with pharmacogenomic or therapeutic-drug-monitoring data, 3D printing enables genuinely personalized regimens. Examples include warfarin titration tablets printed to the exact milligram or transplant patients receiving tacrolimus micro-doses that match real-time trough levels. The technology, therefore, transforms the pharmacist from a distributor of fixed-strength products into a point-of-care manufacturer of bespoke medicines.34-36
Of note, advances in additive manufacturing now allow drug developers to treat each formulation as a malleable digital object rather than a fixed product. This is an outlook that underpins the emerging field of personalized point-of-care pharmacy. Three emerging technological themes stand out. First, multi-material and multilayer printing give pharmacists new levers for controlling dose distribution and release profiles. In a non-pharmaceutical exemplar, Li et al stacked three functional layers (i.e., heater, thermochromic film, and infrared pattern) inside a 140 µm flexible laminate, in which the internal heater raised the surface to 65 °C within 12 seconds, demonstrating that thermal events can be triggered without external hardware.37 Translated to medicines, the same architecture could localize heat-activated drug reservoirs inside dissolvable films, enabling on-skin titration without bulky devices. Second, geometric precision at the microscale and nanoscale can be used to program drug kinetics. Recently, researchers achieved chiral quantum-dot stacks that generated an eight-fold photoluminescence enhancement and a circular dichroism of > 20 ° simply by offsetting 200 nm layers.38 By analogy, offsetting drug-laden strata inside a printable “polypill” might let formulators vary surface area-to-volume ratios or create clockwise versus counter-clockwise helices that modulate dissolution under laminar flow in the gut. Evidence that load-bearing accuracy does not have to be sacrificed comes from Zhang et al, whose continuous-fiber thermoplastic trusses reached an equivalent compression modulus of 402 MPa at a skeletal density of only 1.45 %.39 Such lightweight reinforcement could be embedded in intragastric or intranasal implants without compromising patient comfort. Third, mechanical tuning across wide modulus ranges enables tissue-matched and patient-matched dosage forms. Hong et al printed hydrogel microgel/overlay pairs whose elastic moduli spanned 1.7–31.6 kPa.40 They showed that macrophage spheroid formation and M1/M2 polarization shifted measurably across that gradient, underscoring the biological impact of subtle mechanical cues. For pediatric or geriatric tablets, similar tuning could reconcile the need for structural integrity during handling with rapid disintegration once swallowed. Wattanaanek et al reported on another quantitative anchor. These researchers showed that calcium-phosphate/sulfate scaffolds with 20 wt % ceramic phase could result in a compressive strength of 5.6 MPa, which is well within cancellous-bone territory while supporting MC3T3-E1 proliferation at day 7. The result hints that printable matrices can be strong enough for load-bearing yet porous enough for cell ingress, a duality crucial to long-acting depot systems.41
Layer-by-layer deposition, however, introduces path-length mismatches and residual stresses that can perturb content uniformity. Nakajima and Matsuzaki showed that a 6 ° filament twist minimized the width variation of carbon-fiber plies in curved laminates, reducing cross-sectional error below 0.05 mm. Such optimization is directly relevant to curved orodispersible films intended to sit against the palate.42 At the microscale, Dai et al modelled a selective-laser-melted AlN/AlSi10Mg composite. They found that the dominant heat-flow vector flips from vertical to horizontal after five deposited layers, by which the extension API stability can change continuously during a build and must be captured in process-analytical technology.43
Collectively, these quantitative demonstrations outside traditional pharmaceutics foreshadow a near-term future in which pharmacists exploit the same engineering knobs (e.g., multilayer stacking, mechanical anisotropy, nanoscale patterning) to print medicines whose dose, shape and performance are matched to the physiology and lifestyle of each patient. The challenge now is less about inventing new printers than about translating proven material and process controls into pharmaceutically acceptable inks and establishing regulatory pathways that treat every build file as a controlled but modifiable master record.
While POCT has garnered significant attention as a valuable diagnostic tool in pharmacy settings, 3D printing (also referred to as additive manufacturing) is emerging as another pivotal technology. Although none of the cited studies explicitly address 3D printing in pharmacy, the rapid innovation trajectory in pharmaceutical sciences indicates that 3D printing will likely become more prominent.44 In particular, 3D printing has been recognized for its potential to individualize medication dosages, create complex drug formulations, and fabricate pharmaceutical devices with high levels of customization. In this regard, faculty might face a multifaceted learning curve when asked to teach technologies such as POCT, 3D drug printing, and other emerging advancements.
First, few pharmacy programs cover additive manufacturing, clinical genomics, or near-patient diagnostics. In most programs, the baseline technical literacy appears to be uneven. Faculties also lack such capacity. Bringing them up to speed demands extensive continuing‐education courses, vendor-specific certificates, or even sabbaticals in engineering or clinical laboratories – a commitment that may collide with already heavy teaching, research, and service loads.
Second, hands-on mastery requires access to functioning printers, clean-room space, and a CLIA-waived device. Nonetheless, many colleges lack the capital budget or infrastructure (e.g., ventilation, GMP-compliant workflows) to create and maintain these specialized environments. Additionally, the value may not be viewed as universal at this current time.
Third, curricular time is finite, weaving new competencies into skills labs or therapeutics modules often forces difficult trade-offs with legacy content, and consensus on what to trim is challenging. Also, the issue arises where in the curriculum this is best taught, and what supplemental instruction should be complemented.
Fourth, aligning pedagogy with challenging regulatory frameworks adds complexity. Hence, faculty must teach not only device operation but also documentation practices, process validation, and quality-control metrics that mirror the FDA/EMA standards, which are areas outside traditional pharmacy expertise.
Fifth, educational assessment tools are still emerging; developing objective structured clinical examinations (OSCEs), simulation scenarios, and rubric-based evaluations that accurately capture students’ diagnostic accuracy or printing proficiency can take multiple semesters of iteration.
Finally, many faculty might feel unprepared to lead these endeavors as the technology is state-of-the-art, and many institutions might struggle to reward the extra effort of faculty as promotion criteria seldom credit time spent on technology acquisition, protocol writing, or interdepartmental coordination. Such effects might create disincentives and delays for faculty to champion these innovations unless leadership embeds them in strategic plans and workload models and provides adequate training and development. Perhaps, an innovative solution might be certificate-based education after graduation for faculty.44
Contemporary considerations for POCT and 3D printing
Point-of-care sensory system testing and on-demand 3D printing operate on the same transformative principle, moving critical health-care functions from distant facilities directly into the pharmacy, providing immediate and widespread access, even though they are yet to be refined at different steps of the therapeutic pathway.45,46 With POCT, pharmacists obtain diagnostic data within minutes, enabling same-visit therapeutic decisions that replace the traditional lag created by off-site laboratories. With 3D printing, pharmacists fabricate patient-specific medicines – whether low-dose pediatric formulations, polypills, or modified-release designs – within hours, eliminating lengthy wait times for special-order products or dose splitting that can compromise accuracy. Together, these technologies substantially improve the diagnosis-to-treatment timeline, extend the pharmacist’s clinical scope, and support genuine precision medicine by pairing real-time analytics with custom-built drug fabrication in one accessible location.46 Compared with centralized testing and conventional tablet production, these technologies collectively shorten time to treatment, enhance precision, and position pharmacists at the center of personalized care. Table 2 compares POCT and 3D printing to traditional methods or other technologies, clarifying their unique value in pharmacy.
Table 2.
Comparison of POCT and 3D printing with the traditional methods
|
Criterion
|
POCT
|
3D printing of medicines
|
Traditional methods
|
Unique value added
|
Ref.
|
| Primary use |
Fast, near-patient diagnostics (e.g., HbA1c, influenza, INR) |
On-demand fabrication of dosage forms with tailored dose, shape, or release |
Central laboratory testing/mass tablet manufacturing |
Moves critical steps (diagnosis or compounding) from remote facilities to the pharmacy counter, shortening therapeutic cycles |
46-51
|
| Turn-around time |
≤ 5–30 min from sample to result |
Hours to < 1 day from order to finished dose |
1–3 days for sending-out labs; weeks–months for industrial batch manufacturing |
Accelerates clinical decision-making (POCT) and eliminates wait-time for special-strength or pediatric doses (3DP) |
46,49,51
|
| Location of operation |
Community or hospital pharmacies using CLIA-waived devices |
Hospital or academic pharmacy clean room or Bio-GMP pod |
Central labs / off-site compounding; large GMP plants |
Decentralized services, improving access in rural or understaffed settings |
52,53
|
| Personalization capability |
Limited—interprets patient status, but does not change drug itself |
High—precise milligram-level dose titration, geometry-controlled release, polypills |
Minimal—fixed commercial strengths; split/crush introduces error |
True precision therapeutics: diagnostic result + bespoke dose produced under one roof |
46,51
|
| Typical capital outlay |
US $2 k–20 k per device |
US $20 k–250 k per printer + formulation software |
N/A to individual pharmacy |
Lower entry cost for diagnostics; scalable investment for compounding innovation |
49,54
|
| Regulatory framework |
CLIA-waived/moderate complexity; state pharmacy boards |
FDA/CDER guidance (2017); EMA reflection paper (2023) on personalized meds |
Established compendial standards; ANDA/NDA pathways |
Provides evolving, pharmacy-adapted pathways versus rigid industrial rules |
49,52,54,55
|
| Staff skill set required |
Sample handling, quality control, CLIA documentation |
CAD, extrusion or powder-bed operation, in-process QA |
Routine dispensing, lab logistics |
Drives new competencies that expand pharmacists’ clinical and technological roles |
56
|
| Key implementation barriers |
Reimbursement variability; QC proficiency maintenance |
Raw-material sourcing, printer validation, stability data, cost recovery |
Scale inflexibility, long supply chain |
Overcomes limitations of batch economics and slow feedback loops |
|
GMP: Good Manufacturing Practice, Bio-GMP: biological GMP, CLIA: Clinical Laboratory Improvement Amendments, FDA: Food and Drug Administration (U.S.), CDER: Center for Drug Evaluation and Research, EMA: European Medicines Agency, NDA: Abbreviated New Drug Application, ANDA: Abbreviated NDA, CAD: Computer aided design.
United States FDA and European Union EMA pathways for POCTs
In the U.S., most pharmacy-run POCT systems enter the market as medical devices via 510(k) clearance pathway or, when no suitable predicate exists, a De Novo route. After clearance, sponsors may further file a CLIA-waiver application. To succeed, they must show that untrained users in two independent sites can operate the device safely and similarly to generate results equivalent to a central laboratory.
FDA’s most recent performance metrics put the mean 510(k) decision time at roughly 150 days and dual 510(k)/CLIA submissions at a similar scale, while De Novo reviews average just over 300 days.57,58
Europe regulates the same products under the In-Vitro Diagnostic Regulation (EU) 2017/746. Near-patient assays typically fall in Class C, which obliges manufacturers to undergo a full Notified-Body conformity assessment that commonly spans 9–12 months; transitional provisions adopted in 2024 extend mandatory IVDR compliance for legacy devices to 2027-2029 to relieve capacity constraints.59,60
Across both regions, the principal post-market challenges are economic rather than technical. As a result, pharmacies must finance ongoing quality-control programs and negotiate reimbursement mechanisms that still favor centralized testing.
For additively manufactured medicines, FDA currently applies existing pharmaceutical frameworks while it refines a bespoke policy. Centrally produced products, exemplified by the porous levetiracetam tablet Spritam®, follow the standard NDA or ANDA path, supported by the 2017 guidance titled “Technical Considerations for Additive-Manufactured Medical Devices,” which outlines chemistry-manufacturing-controls expectations for layer-by-layer builds.61
To stimulate innovation, the agency launched an Advanced Manufacturing Technology (AMT) designation program in 2024 that offers enhanced dialogue and prioritized review for distributed-manufacturing platforms, including in-pharmacy printers.62 A separate 2023 discussion paper explores how point-of-care printing might be regulated, suggesting models that range from full NDA oversight to a new “production site” registration category.63 The EMA has flagged similar issues: its network strategy documents and policy analyses identify 3-D printing as a priority technology and note that personalized printlets will still require a Marketing Authorization unless they are prepared under tightly defined magistral exemptions, leaving Member States to harmonize Good Manufacturing Practice expectations.64,65 Review clocks seems to remain comparable to the traditional products, i.e., 10 months (standard), or 6 months (priority) for an NDA in the U.S., and 210 days scientific time in the EU’s centralized procedure. However, both agencies now ask sponsors to justify how they will define “batch,” monitor in-process layer quality, and prove long-term stability for highly porous dosage forms. Such chemistry and GMP hurdles, rather than dossier timelines, are the rate-limiting steps for bringing pharmacy-printed medicines to clinical practice.
Comparative overview of commonly used 3D printing methods in pharmaceutical formulations
Some 3D printing methods are commonly used in the printing process of pharmaceuticals. Depending on the formulation process, different 3D printing techniques can be implemented. The process relies on various techniques, each with distinct advantages, limitations, and application domains.35 Among the most prominent methods are fused deposition modeling (FDM), selective laser sintering (SLS), and inkjet printing.66
Of these, FDM uses a heated nozzle to melt and deposit thermoplastic filaments that may contain active pharmaceutical ingredients (APIs). It is widely adopted due to the availability of low-cost printers and straightforward processes.67 FDM allows for high drug-loading capacity and the fabrication of polypills for personalized therapies.68 However, the elevated processing temperature can degrade heat-sensitive drugs and require pre-processing of filaments (i.e., via hot-melt extrusion), which can introduce complexity.69 FDM has been especially useful for solid oral dosage forms, pediatric formulations, and implants.14
Notably, SLS, as a powder-based process, implements a laser to selectively fuse powdered materials layer by layer.70 One advantage is that the unfused powder acts as a support structure, making it possible to create complex shapes without additional scaffolding.71 This opens the door for intricate geometries and multi-layer drug delivery devices. Nonetheless, the high cost of laser equipment and the need for carefully controlled powder handling can be drawbacks.66 SLS is frequently explored for implantable devices, novel controlled-release systems, and drug-loaded scaffolds.71
Inkjet Printing, on the other hand, precisely deposits small droplets of a solution or suspension containing the drug and excipients onto a substrate.8 It offers exceptional control over dose accuracy and is well-suited for rapidly disintegrating films or personalized dosage forms.72 This method also minimizes material waste. The primary challenges are the strict viscosity and surface tension requirements of the ink, as well as the relatively slow printing speed.70 Altogether, of the FDM, SLS, and Inkjet printing methods, each presents unique benefits for personalized medicine, complex geometries, and controlled release. As research advances, it is increasingly evident that a combination of material innovation, process optimization, and regulatory clarity will drive these technologies toward broader adoption in pharmaceutical education and practice.
The first real-world evidence comes from Spritam® (levetiracetam), the epilepsy medicine that became the inaugural FDA-approved 3D-printed tablet in 2015. Produced with Aprecia’s ZipDose® powder-bed technology, the printlets possess a highly porous architecture that disperses in seconds with a sip of water, removing a well-known swallowing barrier for high-strength antiepileptic drugs. Post-approval pharmacovigilance reports compiled by hospital pharmacies have linked the rapid-dissolve profile to better dose completion in pediatric and geriatric populations and fewer crushing/splitting errors during medication administration.50,73 Clinicians also point to the formulation’s precise layer-by-layer dosing as an aid to therapeutic drug monitoring, because each unit contains the full labeled amount without the variability sometimes seen in split tablets. Together, these operational gains illustrate how an FDA-cleared 3D-printed product can outperform conventional solid doses in daily pharmacy practice. Complementary data are emerging from hospital-based trials that fabricate personalized medicines on site. In Finland, semisolid-extrusion printers were used to create orodispersible warfarin films in four pediatric strengths (0.1–2 mg) and compared head-to-head with the pharmacy’s traditional oral-powder sachets. The printed films met European Pharmacopoeia content-uniformity limits. The products showed tighter dose accuracy than the compounded powders while remaining physically stable for one month and fully dispersing in water. These products are attributed to having streamlined anticoagulation management on the pediatric ward. A separate single-center crossover study in Spain provided chewable amino-acid printlets for children with inherited metabolic disorders. Remarkably, the 3D-printed formulations kept plasma citrulline and branched-chain amino-acid levels within target ranges and were preferred in taste tests, supporting improved adherence.46,51
Challenges and considerations
Despite the promise of 3D printing, several practical issues must be addressed before it becomes widely integrated in pharmacy education. The cost of acquiring and maintaining the necessary hardware, software, and materials can be substantial.27 Additionally, establishing robust quality assurance protocols and ensuring regulatory compliance require a comprehensive framework that spans both academic institutions and licensing bodies.25
Training faculty and students to use 3D printing equipment effectively is also pivotal. Educators may need to develop specialized teaching modules and collaborate with experts in engineering or industrial design to incorporate best practices.4 Similar to POCT training, where students must learn how to operate devices and interpret results accurately,2 3D printing education would require a thorough understanding of digital design software, polymer science, and drug stability considerations.
Implications for curriculum development
As both POCT and 3D printing gain traction, pharmacy education must evolve to include competencies that align with these emerging technologies. Curricula may incorporate interdisciplinary coursework covering diagnostics, clinical interpretation, product design, and patient-centered services. For POCT, integrating classroom learning with hands-on experience ensures that students are prepared to perform and interpret tests confidently upon entering practice.6 For 3D printing, schools could offer laboratory-based modules that guide students through the design, production, and testing of printed dosage forms, thereby connecting theoretical content with real-world applications.44
Collaboration with industry, regulatory agencies, and professional organizations is essential for shaping educational standards. Similar to how organizations have advocated for increased POCT training to expand pharmacists’ clinical impact,2 it is anticipated that these same entities will promote policies and guidelines around 3D printing to ensure safety, efficacy, and ethical considerations.1 Incorporating these guidelines into coursework and experiential learning helps students remain up to date with evolving practice standards.
Finally, the incorporation of POCT and 3D printing must be undertaken with attention to resource allocation and faculty expertise.74 While advanced technologies can enhance learning, they also require investment in physical infrastructure, curriculum redesign, and continuing education for instructors. Optimizing these elements ensures that the next generation of pharmacists is well-equipped to harness the full potential of emerging tools in patient care.
The integration of POCT and 3D printing into pharmacy education underscores the ongoing transformation of the profession. Of these, POCT has already demonstrated its value in expanding pharmacists’ roles, from infectious disease screening to chronic disease management.26,27 Meanwhile, 3D printing stands at the frontier of personalized medicine and drug formulation, offering students an immersive way to understand complex pharmaceutical concepts and novel manufacturing processes.44 By aligning educational practices with these advancing technologies, pharmacy programs can better prepare graduates to meet contemporary healthcare challenges, improve patient outcomes, and spearhead innovations in drug delivery and diagnostics. As these technologies continue to evolve, ongoing collaboration between educators, regulatory bodies, and practice leaders will be essential to ensure that the pharmacy profession remains responsive to the needs of patients and the broader healthcare system.
Key highlights in 3D and 4D printing to regenerate tissues
In precision regenerative medicine, 3D and 4D printing are rapidly revolutionizing tissue regeneration by enabling the fabrication of complex, patient-specific constructs that closely mimic native tissue architecture. Traditional 3D bioprinting allows for the accurate placement of cells and biomaterials—often hydrogels like alginate, collagen, or PEG-based polymers—to form scaffolds with tailored mechanical properties and biological cues.75 A notable success includes achieving a compressive modulus of 0.38 MPa in double-network hydrogels, sufficient for many soft tissues.76 Another significant advance is the incorporation of nanomaterials (e.g., graphene oxide, zinc-doped hydroxyapatite) for enhancing both osteogenic differentiation and antibacterial activity by up to 3.4 times.77 In contrast, 4D printing introduces a temporal component whereby materials or constructs change shape or properties upon exposure to specific stimuli, such as temperature or pH.78 This dynamic capability is important for tissues undergoing continuous mechanical or biochemical changes, including cartilage or vascular grafts. Targeted cell placement further boosts the functionality of printed structures. For example, aspiration-assisted bioprinting enabled spheroid placement with an 11% margin relative to each spheroid’s diameter, promoting scaffold-free bone growth.79 Despite these advances, challenges persist. Vascularization of large printed constructs, ensuring regulatory compliance, and controlling print fidelity across different scales remain crucial priorities.80 Cost and scalability issues also limit widespread clinical adoption. Still, as collaborative research integrates advanced bioink formulations, smart stimuli-responsive materials, and refined printing hardware, 3D and 4D printing stand poised to deliver transformative solutions for personalized tissue repair and regeneration.
Personalized formulations and bioinks
While 3D printing initially gained traction in manufacturing and surgical planning, its adaptation in tissue engineering and regenerative medicine has opened new avenues wherein pharmacists can play a pivotal role in optimizing therapeutic outcomes and ensuring patient safety.80 At the heart of 3D and 4D printing are bioinks, which are complex formulations typically composed of hydrogels, cells, and various bioactive components.75 Pharmacists bring extensive expertise in compounding and formulation design, making them central to ensuring that the final scaffold or printed tissue is produced under stringent quality standards. For instance, novel hydrogels, including thermoresponsive polymers or composite materials doped with antibacterial agents, must be carefully characterized for stability, sterility, biocompatibility, and consistency.81 In this context, pharmacists can contribute to selecting excipients or crosslinkers that minimize toxicity or immune responses, thereby advancing patient-specific treatments that integrate seamlessly into a patient’s therapeutic regimen. Fig. 3 represents the impacts and applications of bioinks in the development of precision medicine.
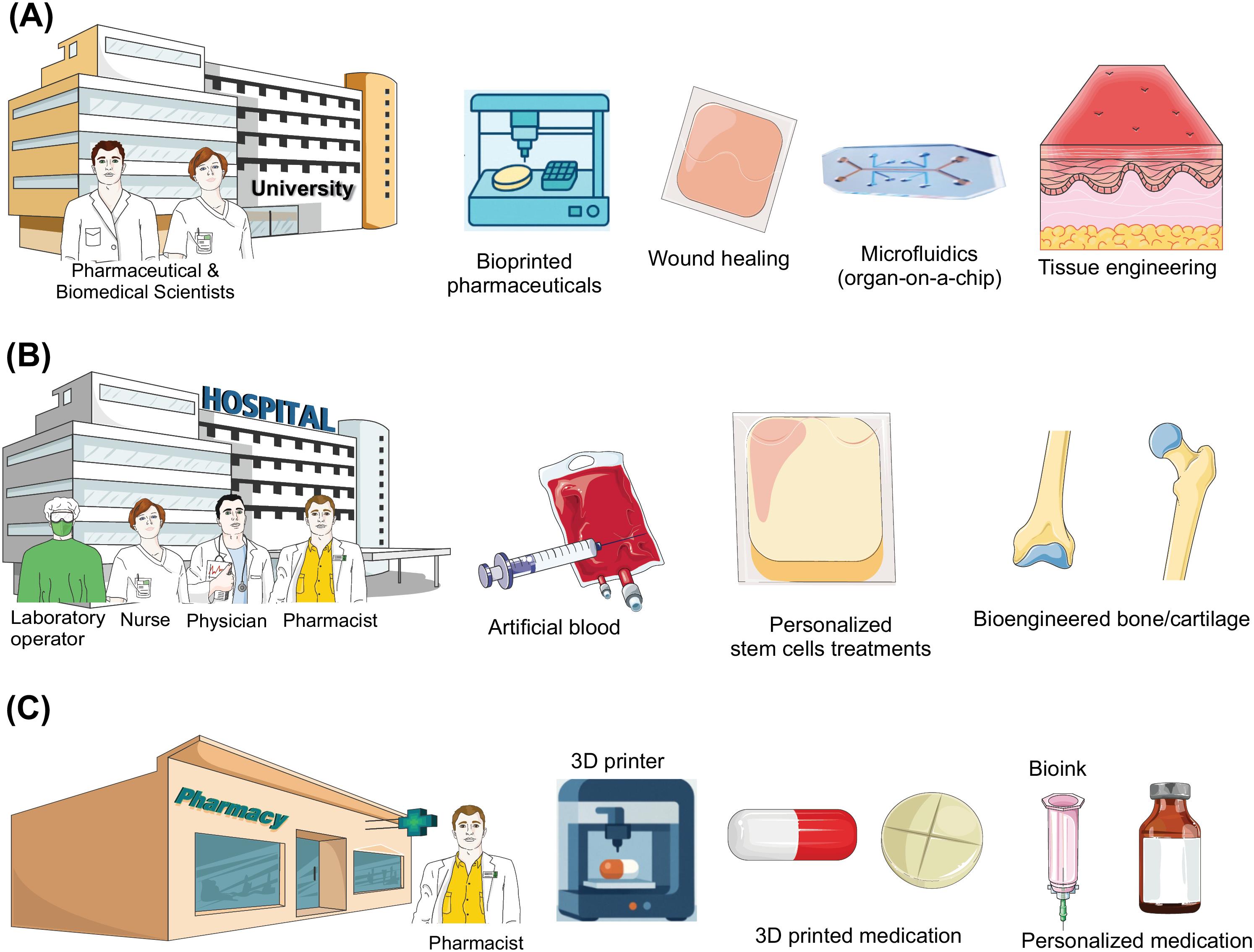
Fig. 3.
Schematic illustration of the impacts and applications of advanced technologies (e.g., 3D prinitin, bioinks, etc) in the development of precision medicine. A) Universities and pharmaceutical industries initiate AI-assisted research and development of personalized medicine utilizing technolgies like microfluidics technology integrated with 3D printing using active pharmaceutical ingredients, excipients, and hydrogel incorporated with different entities. B) Major applications of bioinks in hospitals - a collaborative approach among medical doctors and pharmacists. (C) Futuristic pharmacy involved with new technologies such as 3D printing and bioinks for patient-specific services.
.
Schematic illustration of the impacts and applications of advanced technologies (e.g., 3D prinitin, bioinks, etc) in the development of precision medicine. A) Universities and pharmaceutical industries initiate AI-assisted research and development of personalized medicine utilizing technolgies like microfluidics technology integrated with 3D printing using active pharmaceutical ingredients, excipients, and hydrogel incorporated with different entities. B) Major applications of bioinks in hospitals - a collaborative approach among medical doctors and pharmacists. (C) Futuristic pharmacy involved with new technologies such as 3D printing and bioinks for patient-specific services.
This technology is necessary for the development of advanced cell-based products. The expanding scope of regenerative medicine involves the integration of stem cells, growth factors, and gene therapy components into printed constructs. Pharmacists are often responsible for handling biological products, adhering to best practices for storage, transport, and aseptic processing. As 3D-printed constructs become more “drug-like”—for example, incorporating biomolecules such as growth factors (BMP-4, VEGF) or antibiotics—pharmacists must collaborate with biomedical teams to evaluate dosing schedules, stability profiles, and interactions with other medications the patient may be taking.79 Their skills in pharmacokinetics and pharmacodynamics will be vital in determining optimal release profiles that maximize regenerative outcomes while minimizing side effects.
Given that many 3D and 4D printed tissues and scaffolds involve living cells, these products align with biologics or advanced therapy medicinal products (ATMPs) categories.80 Pharmacists, through their familiarity with good manufacturing practices (GMP) and regulatory frameworks (e.g., FDA, EMA), can guide product development to ensure compliance. This extends to validating the sterility and reproducibility of printed constructs, conducting risk assessments, and managing documentation. In addition, ongoing pharmacovigilance monitoring for adverse reactions post-implantation becomes a shared responsibility for clinicians and pharmacists, especially in the early commercialization stages of these new therapies.
Clinical and translational collaboration is another essential dimension in interprofessional approaches. Pharmacists, clinicians, biologists, bioengineers, and researchers must work closely to bring 3D- and 4D-printed therapies to patients. Pharmacists, with their deep understanding of formulations and drug-device combination products, can champion translational research that seeks to streamline the path from bench to bedside.82 This includes designing stability studies, evaluating packaging, advising on cold-chain logistics for cell-laden formulations, and participating in multi-disciplinary teams tasked with clinical trial design and execution. As these technologies mature, the pharmacy profession will likely see an expansion in roles such as “bioprinting pharmacists,” who specialize in customizing bioinks and scaffolds in hospital-based or centralized compounding facilities. Strengthening educational curricula around biotechnology and additive manufacturing will thus be crucial. Additionally, ethical considerations, for instance, equitable access and long-term implant monitoring, will become central to practice guidelines, where pharmacists can offer leadership in policy-making and patient advocacy. Taken all, 3D and 4D printing technologies represent a transformative frontier for tissue regeneration and personalized healthcare. Pharmacists, recognized for their roles in formulation science, quality control, and patient-centric care, stand at the nexus of scientific discovery and clinical application. By leveraging their expertise, the pharmacy profession can drive safe, effective, and sustainable integration of these emerging regenerative therapies into standard healthcare practices.
Conclusion
Advancements in POCT and 3D printing are reshaping both the practice and education of pharmacists. POCT extends the scope of community and clinical pharmacy services by enabling swift, onsite diagnostic capabilities. Simultaneously, 3D printing introduces a novel dimension to pharmaceutical science, particularly in drug formulation and personalized medicine. The capacity to design and produce tailored dosage forms addresses individual patient needs such as dose specificity, ease of administration, and improved adherence. Nevertheless, harnessing this potential requires pharmacy education to incorporate laboratory instruction and interdisciplinary learning experiences, merging principles of pharmaceutics, engineering, and patient-centric care. With adequate institutional support, faculty training, and infrastructure, students can gain an experiential understanding of the entire 3D printing process, from conceptualization to quality assurance.
Overall, the successful adoption of POCT and 3D printing in pharmacy depends on strategic curriculum development, ongoing faculty development, and robust collaborations with external stakeholders such as healthcare institutions, policymakers, and industry partners. By embracing these emerging technologies and seamlessly integrating them into educational frameworks, the pharmacy profession is poised to assume an expanded role in primary and specialty care. This evolution not only benefits patient outcomes but also elevates the pharmacist’s position as a dynamic healthcare provider, innovator, and integral member of multidisciplinary teams.
Review Highlights
What is the current knowledge?
-
Point-of-care testing (POCT) systems have been marketed for monitoring of some diseases such as diabetes.
-
3D printing personalizes dosage forms, enhancing therapy in pharmacy practice.
-
Various printing methods (FDM, SLS, Inkjet) are widely researched for drug development.
-
Biodegradable polymers offer eco-friendly solutions and reduce toxicity risks.
-
Regulatory frameworks for 3D printing in pharma are evolving but still lack clear guidelines.
-
Pharmacists can use 3D printing to tailor pediatric, geriatric, and specialty treatments.
What is new here?
-
Personalized POCT systems is a turnaround approach in controlling diseases by patients.
-
The use of POCT as an early disease detection approach results in rapid intervention.
-
The AI-driven design optimizes 3D-printed formulations for individualized patient needs.
-
On-demand printing in pharmacies enables faster, personalized drug dispensing.
-
Smart inhalers and implants can be custom-made via advanced 3D printing methods.
-
SLA and multi-nozzle printers expand complex geometries for targeted drug release.
-
Data-enriched tablets integrate dosing info and QR codes for safer medication use.
-
Microfluidic-based bioprinting refines vascularization and nutrient flow in large tissue constructs.
-
AI-driven slicing optimizes print paths, boosting efficiency, cell viability, and design complexity.
Competing Interests
The authors declare that they have no conflict of interest regarding this work.
Ethical Approval
None to be stated.
Acknowledgements
The authors are thankful for Nova Southeastern University's support.
References
- Banfi G, Bozic B, Cihan M, Pasalic D, Pennestri F, Plebani M. Point-of-care testing, near-patient testing and patient self-testing: warning points. Clin Chem Lab Med 2024; 62:2388-92. doi: 10.1515/cclm-2024-0525 [Crossref] [ Google Scholar]
- Gallimore CE, Porter AL, Barnett SG, Portillo E, Zorek JA. A state-level needs analysis of community pharmacy point-of-care testing. J Am Pharm Assoc (2003) 2021; 61:e93-e8. doi: 10.1016/j.japh.2020.12.013 [Crossref] [ Google Scholar]
- Sun Z, Qing M, Fan YZ, Yan H, Li NB, Luo HQ. Quadruple analyte responsive platform: Point-of-care testing and multi-coding logic computation based on metal ions recognition and selective response. J Hazard Mater 2022; 437:129331. doi: 10.1016/j.jhazmat.2022.129331 [Crossref] [ Google Scholar]
- Hutchings L, Shiamptanis A. Evaluation of Point-of-Care Testing in Pharmacy to Inform Policy Writing by the New Brunswick College of Pharmacists. Pharmacy (Basel) 2022; 10:159. doi: 10.3390/pharmacy10060159 [Crossref] [ Google Scholar]
- McKeirnan K, Czapinski J, Bertsch T, Buchman C, Akers J. Training Student Pharmacists to Perform Point-of-Care Testing. Am J Pharm Educ 2019; 83:7031. doi: 10.5688/ajpe7031 [Crossref] [ Google Scholar]
- Staudt AM, Draime JA, Deitschmann N, Norfolk M, Jenkins ZN. Training student pharmacists to facilitate human immunodeficiency virus point-of-care testing. Curr Pharm Teach Learn 2020; 12:1245-51. doi: 10.1016/j.cptl.2020.05.004 [Crossref] [ Google Scholar]
- Bury D, Martin-Hirsch PL, Martin FL, Dawson TP. Are new technologies translatable to point-of-care testing?. Lancet 2017; 390:2765-6. doi: 10.1016/S0140-6736(17)33301-9 [Crossref] [ Google Scholar]
- Carou-Senra P, Rodriguez-Pombo L, Awad A, Basit AW, Alvarez-Lorenzo C, Goyanes A. Inkjet Printing of Pharmaceuticals. Adv Mater 2024; 36:e2309164. doi: 10.1002/adma.202309164 [Crossref] [ Google Scholar]
- Chakka LRJ, Chede S. 3D printing of pharmaceuticals for disease treatment. Front Med Technol 2022; 4:1040052. doi: 10.3389/fmedt.2022.1040052 [Crossref] [ Google Scholar]
-
Mathew E, Pitzanti G, Larraneta E, Lamprou DA. 3D Printing of Pharmaceuticals and Drug Delivery Devices. Pharmaceutics 2020; 12. doi: 10.3390/pharmaceutics12030266.
- Ahmed TA, Felimban RI, Tayeb HH, Rizg WY, Alnadwi FH, Alotaibi HA. Development of Multi-Compartment 3D-Printed Tablets Loaded with Self-Nanoemulsified Formulations of Various Drugs: A New Strategy for Personalized Medicine. Pharmaceutics 2021; 13:1733. doi: 10.3390/pharmaceutics13101733 [Crossref] [ Google Scholar]
- Medina C, Richmond FJ. Incentivizing Quality in the Manufacture of Pharmaceuticals: Industry Views on Quality Metrics and Ratings. TherInnovRegul Sci 2015; 49:730-8. doi: 10.1177/2168479015589821 [Crossref] [ Google Scholar]
- Mirza MA, Iqbal Z. 3D Printing in Pharmaceuticals: Regulatory Perspective. Curr Pharm Des 2018; 24:5081-3. doi: 10.2174/1381612825666181130163027 [Crossref] [ Google Scholar]
- Pawar R, Pawar A. 3D printing of pharmaceuticals: approach from bench scale to commercial development. Futur J Pharm Sci 2022; 8:48. doi: 10.1186/s43094-022-00439-z [Crossref] [ Google Scholar]
- Hagemeier NE, Murawski MM. Junior pharmacy faculty members' perceptions of their exposure to postgraduate training and academic careers during pharmacy school. Am J Pharm Educ 2012; 76:39. doi: 10.5688/ajpe76339 [Crossref] [ Google Scholar]
- Wanat MA, Fleming ML, Fernandez JM, Garey KW. Education, training, and academic experience of newly hired, first-time pharmacy faculty members. Am J Pharm Educ 2014; 78:92. doi: 10.5688/ajpe78592 [Crossref] [ Google Scholar]
- Wilbur K, Paiva M, Black E. Pharmacy Student and Preceptor Impressions of Faculty Liaison Visits to Experiential Training Sites. Am J Pharm Educ 2015; 79:134. doi: 10.5688/ajpe799134 [Crossref] [ Google Scholar]
-
Zimmermann AE, Thomas MC. Essential Training, Resources, and Skills of First-Year and Junior Pharmacy Practice Faculty Needed in the Development of an Individual Research Program. J Pharm Pract 2017; 897190017731244. doi: 10.1177/0897190017731244.
- Obarcanin E, Aslani P, Ho AHY, Bandiera C, Baysari M, Bojic I. Exploring research and education opportunities in digital health for pharmacy, medicine and other health disciplines: Insights from a multinational workshop. Explor Res Clin Soc Pharm 2024; 15:100469. doi: 10.1016/j.rcsop.2024.100469 [Crossref] [ Google Scholar]
- Kinny F, Schlottau S, Ali Sherazi B, Obarcanin E, Laer S. Digital health in pharmacy education: Elective practical course integrating wearable devices and their generated health data. Explor Res Clin Soc Pharm 2024; 15:100465. doi: 10.1016/j.rcsop.2024.100465 [Crossref] [ Google Scholar]
- Wong JC, Hekimyan L, Cruz FA, Brower T. Identifying Pertinent Digital Health Topics to Incorporate into Self-Care Pharmacy Education. Pharmacy (Basel) 2024; 12:96. doi: 10.3390/pharmacy12030096 [Crossref] [ Google Scholar]
- Omidian H, Omidi Y. Blockchain in pharmaceutical life cycle management. Drug Discov Today 2022; 27:935-8. doi: 10.1016/j.drudis.2022.01.018 [Crossref] [ Google Scholar]
- Lee S, Bi L, Chen H, Lin D, Mei R, Wu Y. Recent advances in point-of-care testing of COVID-19. Chem Soc Rev 2023; 52:8500-30. doi: 10.1039/d3cs00709j [Crossref] [ Google Scholar]
- Zhang Y, Zhang B, Guo Z, Lu S, Li Y, Zhang R. A miniaturized colorimetric-photoacoustic dual-mode device for point-of-care testing of ascorbic acid and ascorbate oxidase. Anal Chim Acta 2025; 1341:343685. doi: 10.1016/j.aca.2025.343685 [Crossref] [ Google Scholar]
- Essack S, Bell J, Burgoyne D, Tongrod W, Duerden M, Sessa A. Point-of-Care Testing for Pharyngitis in the Pharmacy. Antibiotics (Basel) 2020; 9:743. doi: 10.3390/antibiotics9110743 [Crossref] [ Google Scholar]
- McKeirnan K, Kherghehpoush S, Gladchuk A, Patterson S. Addressing Barriers to HIV Point-of-Care Testing in Community Pharmacies. Pharmacy (Basel) 2021; 9:84. doi: 10.3390/pharmacy9020084 [Crossref] [ Google Scholar]
- Min AC, Andres JL, Grover AB, Megherea O. Pharmacist Comfort and Awareness of HIV and HCV Point-of-Care Testing in Community Settings. Health PromotPract 2020; 21:831-7. doi: 10.1177/1524839919857969 [Crossref] [ Google Scholar]
- Akbari Nakhjavani S, Khalilzadeh B, Afsharan H, Hosseini N, Ghahremani MH, Carrara S. Electrochemiluminescent immunosensor for detection of carcinoembryonic antigen using luminol-coated silver nanoparticles. Mikrochim Acta 2023; 190:77. doi: 10.1007/s00604-023-05656-8 [Crossref] [ Google Scholar]
- Johari-Ahar M, Rashidi MR, Barar J, Aghaie M, Mohammadnejad D, Ramazani A. An ultra-sensitive impedimetric immunosensor for detection of the serum oncomarker CA-125 in ovarian cancer patients. Nanoscale 2015; 7:3768-79. doi: 10.1039/c4nr06687a [Crossref] [ Google Scholar]
- Hosseini N, Akbari Nakhjavani S, Ardalan M, Salimi A, Mirzajani H, Adibkia K. Unlocking diagnostic potential: Advances in biosensing platforms for detection of cystatin C, a kidney disease biomarker. Microchem J 2025; 210:113032. doi: 10.1016/j.microc.2025.113032 [Crossref] [ Google Scholar]
- Akbari Nakhjavani S, Afsharan H, Khalilzadeh B, Ghahremani MH, Carrara S, Omidi Y. Gold and silver bio/nano-hybrids-based electrochemical immunosensor for ultrasensitive detection of carcinoembryonic antigen. BiosensBioelectron 2019; 141:111439. doi: 10.1016/j.bios.2019.111439 [Crossref] [ Google Scholar]
- Akbari Nakhjavani S, Khalilzadeh B, Samadi Pakchin P, Saber R, Ghahremani MH, Omidi Y. A highly sensitive and reliable detection of CA15-3 in patient plasma with electrochemical biosensor labeled with magnetic beads. BiosensBioelectron 2018; 122:8-15. doi: 10.1016/j.bios.2018.08.047 [Crossref] [ Google Scholar]
- Karami P, Majidi MR, Johari-Ahar M, Barar J, Omidi Y. Development of screen-printed tryptophan-kynurenine immunosensor for in vitro assay of kynurenine-mediated immunosuppression effect of cancer cells on activated T-cells. BiosensBioelectron 2017; 92:287-93. doi: 10.1016/j.bios.2016.11.010 [Crossref] [ Google Scholar]
- Singhvi G, Patil S, Girdhar V, Chellappan DK, Gupta G, Dua K. 3D-printing: an emerging and a revolutionary technology in pharmaceuticals. Panminerva Med 2018; 60:170-3. doi: 10.23736/S0031-0808.18.03467-5 [Crossref] [ Google Scholar]
- Trenfield SJ, Awad A, Goyanes A, Gaisford S, Basit AW. 3D Printing Pharmaceuticals: Drug Development to Frontline Care. Trends Pharmacol Sci 2018; 39:440-51. doi: 10.1016/j.tips.2018.02.006 [Crossref] [ Google Scholar]
- Chandekar A, Mishra DK, Sharma S, Saraogi GK, Gupta U, Gupta G. 3D Printing Technology: A New Milestone in the Development of Pharmaceuticals. Curr Pharm Des 2019; 25:937-45. doi: 10.2174/1381612825666190507115504 [Crossref] [ Google Scholar]
- Li Z, Li Y, Zhou M, Zhu X, Wang R, Zhang YF. 3D printing of thermochromic multilayer flexible film for multilevel information encryption. J Colloid Interface Sci 2025; 678:776-88. doi: 10.1016/j.jcis.2024.09.143 [Crossref] [ Google Scholar]
- Kim GY, Kim S, Park KH, Jang H, Kim M, Nam TW. Chiral 3D structures through multi-dimensional transfer printing of multilayer quantum dot patterns. Nat Commun 2024; 15:6996. doi: 10.1038/s41467-024-51179-y [Crossref] [ Google Scholar]
- Zhang D, Tian X, Zhou Y, Wang Q, Yan W, Akmal Zia A. Spatial 3D Printing of Continuous Fiber-Reinforced Composite Multilayer Truss Structures with Controllable Structural Performance. Polymers (Basel) 2023; 15:4333. doi: 10.3390/polym15214333 [Crossref] [ Google Scholar]
- Hong J, Shin Y, Lee J, Cha C. Programmable multilayer printing of a mechanically-tunable 3D hydrogel co-culture system for high-throughput investigation of complex cellular behavior. Lab Chip 2021; 21:710-8. doi: 10.1039/d0lc01230k [Crossref] [ Google Scholar]
- Wattanaanek N, Suttapreyasri S, Samruajbenjakun B. 3D Printing of Calcium Phosphate/Calcium Sulfate with Alginate/Cellulose-Based Scaffolds for Bone Regeneration: Multilayer Fabrication and Characterization. J FunctBiomater 2022; 13:47. doi: 10.3390/jfb13020047 [Crossref] [ Google Scholar]
- Nakajima K, Matsuzaki R. Formability of curved multilayer laminates via 3D printing using twisted continuous fiber composites. Heliyon 2023; 9:e20986. doi: 10.1016/j.heliyon.2023.e20986 [Crossref] [ Google Scholar]
- Dai D, Gu D, Poprawe R, Xia M. Influence of additive multilayer feature on thermodynamics, stress and microstructure development during laser 3D printing of aluminum-based material. Sci Bull (Beijing) 2017; 62:779-87. doi: 10.1016/j.scib.2017.05.007 [Crossref] [ Google Scholar]
- Bright DR, Klepser ME, Murry L, Klepser DG. Pharmacist-Provided Pharmacogenetic Point-of-Care Testing Consultation Service: A Time and Motion Study. J Pharm Technol 2018; 34:139-43. doi: 10.1177/8755122518756651 [Crossref] [ Google Scholar]
- Goodhart A, Johnson H, Bodkins E, Samek K. Impact of Point of Care Hemoglobin A1c Testing on Time to Therapeutic Intervention. J Am Board Fam Med 2024; 37:790-1. doi: 10.3122/jabfm.2023.230425R1 [Crossref] [ Google Scholar]
- Oblom H, Sjoholm E, Rautamo M, Sandler N. Towards Printed Pediatric Medicines in Hospital Pharmacies: Comparison of 2D and 3D-Printed Orodispersible Warfarin Films with Conventional Oral Powders in Unit Dose Sachets. Pharmaceutics 2019; 11:334. doi: 10.3390/pharmaceutics11070334 [Crossref] [ Google Scholar]
- Sjoholm E, Sandler N. Additive manufacturing of personalized orodispersible warfarin films. Int J Pharm 2019; 564:117-23. doi: 10.1016/j.ijpharm.2019.04.018 [Crossref] [ Google Scholar]
- Anonymous. APRECIA Available from: https://aprecia.com/resources/press/fda-approves-the-first-3d-printed-drug-product/.
- Anonymous. PTS Diagnostics. Available from: https://www.ptsdiagnostics.com/a1cnow-systems-overview/.
- Okafor-Muo OL, Hassanin H, Kayyali R, ElShaer A. 3D Printing of Solid Oral Dosage Forms: Numerous Challenges With Unique Opportunities. J Pharm Sci 2020; 109:3535-50. doi: 10.1016/j.xphs.2020.08.029 [Crossref] [ Google Scholar]
- Rodriguez-Pombo L, de Castro-Lopez MJ, Sanchez-Pintos P, Giraldez-Montero JM, Januskaite P, Duran-Pineiro G. Paediatric clinical study of 3D printed personalised medicines for rare metabolic disorders. Int J Pharm 2024; 657:124140. doi: 10.1016/j.ijpharm.2024.124140 [Crossref] [ Google Scholar]
- Anonymous. CDC. Available from: https://www.cdc.gov/clia/php/test-complexities/index.html.
- Anonymous. U.S. FDA. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/technical-considerations-additive-manufactured-medical-devices.
- Anonymous. U.S.FDA. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/technical-considerations-additive-manufactured-medical-devices.
- Anonymous. Towards the European medicines agencies network strategy 2028 (EMANS 2028). Heads of Medicines Agencies(HMA), European Medicines Agency (EMA).
- American Association of Colleges of Pharmacy Faculty Survey 2024 National Summary Report: Available from: https://www.aacp.org/sites/default/files/2024-08/2024-faculty-national-summary-report.pdf.
- Aboy M, Crespo C, Stern A. Beyond the 510(k): The regulation of novel moderate-risk medical devices, intellectual property considerations, and innovation incentives in the FDA's De Novo pathway. NPJ Digit Med 2024; 7:29. doi: 10.1038/s41746-024-01021-y [Crossref] [ Google Scholar]
- FDA US. MDUFA performance goals and procedures, fiscal years 2023 through 20272023: Available from: https://www.fda.gov/about-fda/user-fee-performance-reports/mdufa-performance-reports.
- Commission E. Extension of the IVDR transitional periods2024: Available from: https://health.ec.europa.eu/document/download/dfd7a1c6-f319-4682-9bac-77bef1165818_en.
- Commission E. Commission proposes measures to improve the availability of in vitro diagnostics 2024: Available from: https://ec.europa.eu/commission/presscorner/detail/en/ip_24_346?.
- FDA US. Technical Considerations for Additive Manufactured Medical Devices: Guidance for Industry and Food and Drug Administration Staff. 2018; Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/technical-considerations-additive-manufactured-medical-devices?.
- FDA US. Advanced Manufacturing Technologies Designation Program. 2024; Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/advanced-manufacturing-technologies-designation-program?.
- FDA US. 3D Printing Medical Devices at the Point of Care: Discussion Paper. 2021; Available from: https://www.fda.gov/medical-devices/3d-printing-medical-devices/3d-printing-medical-devices-point-care-discussion-paper?.
- Englezos K, Wang L, Tan ECK, Kang L. 3D printing for personalised medicines: implications for policy and practice. Int J Pharm 2023; 635:122785. doi: 10.1016/j.ijpharm.2023.122785 [Crossref] [ Google Scholar]
- European medicines agencies network strategy. Available from: https://www.ema.europa.eu/en/about-us/how-we-work/european-medicines-regulatory-network/european-medicines-agencies-network-strategy.
- Deng M, Wu S, Ning M. 3D printing for controlled release Pharmaceuticals: Current trends and future directions. Int J Pharm 2025; 669:125089. doi: 10.1016/j.ijpharm.2024.125089 [Crossref] [ Google Scholar]
- Deshkar S, Rathi M, Zambad S, Gandhi K. Hot Melt Extrusion and its Application in 3D Printing of Pharmaceuticals. Curr Drug Deliv 2021; 18:387-407. doi: 10.2174/1567201817999201110193655 [Crossref] [ Google Scholar]
- Moroni S, Khorshid S, Aluigi A, Tiboni M, Casettari L. Poly(3-hydroxybutyrate): A potential biodegradable excipient for direct 3D printing of pharmaceuticals. Int J Pharm 2022; 623:121960. doi: 10.1016/j.ijpharm.2022.121960 [Crossref] [ Google Scholar]
- Somwanshi A, Wadhwa P, Raza A, Hudda S, Magan M, Khera K. Natural Alternatives to Non-biodegradable Polymers in 3D Printing of Pharmaceuticals. Curr Pharm Des 2023; 29:2281-90. doi: 10.2174/0113816128259971230921111755 [Crossref] [ Google Scholar]
- Patel R, Patel S, Shah N, Shah S, Momin I, Shah S. 3D printing chronicles in medical devices and pharmaceuticals: tracing the evolution and historical milestones. J Biomater Sci Polym Ed 2024; 35:2723-66. doi: 10.1080/09205063.2024.2386222 [Crossref] [ Google Scholar]
- Wadher K, Trivedi R, Wankhede N, Kale M, Umekar M. 3D printing in pharmaceuticals: An emerging technology full of challenges. Ann Pharm Fr 2021; 79:107-18. doi: 10.1016/j.pharma.2020.08.007 [Crossref] [ Google Scholar]
- Oblom H, Cornett C, Botker J, Frokjaer S, Hansen H, Rades T. Data-enriched edible pharmaceuticals (DEEP) of medical cannabis by inkjet printing. Int J Pharm 2020; 589:119866. doi: 10.1016/j.ijpharm.2020.119866 [Crossref] [ Google Scholar]
- Li X, Liang E, Hong X, Han X, Li C, Wang Y. In Vitro and In Vivo Bioequivalence Study of 3D-Printed Instant-Dissolving Levetiracetam Tablets and Subsequent Personalized Dosing for Chinese Children Based on Physiological Pharmacokinetic Modeling. Pharmaceutics 2021; 14:20. doi: 10.3390/pharmaceutics14010020 [Crossref] [ Google Scholar]
- Kherghehpoush S, McKeirnan KC. Pharmacist-led HIV and hepatitis C point-of-care testing and risk mitigation counseling in individuals experiencing homelessness. Explor Res Clin Soc Pharm 2021; 1:100007. doi: 10.1016/j.rcsop.2021.100007 [Crossref] [ Google Scholar]
- Dell AC, Wagner G, Own J, Geibel JP. 3D bioprinting using hydrogels: cell inks and tissue engineering applications. Pharmaceutics 2022; 14:2596. doi: 10.3390/pharmaceutics14122596 [Crossref] [ Google Scholar]
- Greco I, Machrafi H, Iorio CS. Double-Network Hydrogel 3D BioPrinting Biocompatible with Fibroblast Cells for Tissue Engineering Applications. Gels 2024; 10:684. doi: 10.3390/gels10110684 [Crossref] [ Google Scholar]
- Maleki-Ghaleh H, Siadati MH, Fallah A, Koc B, Kavanlouei M, Khademi-Azandehi P. Antibacterial and Cellular Behaviors of Novel Zinc-Doped Hydroxyapatite/Graphene Nanocomposite for Bone Tissue Engineering. Int J Mol Sci 2021; 22:9564. doi: 10.3390/ijms22179564 [Crossref] [ Google Scholar]
- Di Marzio N, Eglin D, Serra T, Moroni L. Bio-Fabrication: Convergence of 3D Bioprinting and Nano-Biomaterials in Tissue Engineering and Regenerative Medicine. Front BioengBiotechnol 2020; 8:326. doi: 10.3389/fbioe.2020.00326 [Crossref] [ Google Scholar]
-
Heo DN, Ayan B, Dey M, Banerjee D, Wee H, Lewis GS, et al. Aspiration-assisted bioprinting of co-cultured osteogenic spheroids for bone tissue engineering. Biofabrication 2020; 13. doi: 10.1088/1758-5090/abc1bf.
- Beheshtizadeh N, Gharibshahian M, Pazhouhnia Z, Rostami M, Zangi AR, Maleki R. Commercialization and regulation of regenerative medicine products: Promises, advances and challenges. Biomed Pharmacother 2022; 153:113431. doi: 10.1016/j.biopha.2022.113431 [Crossref] [ Google Scholar]
- Amiryaghoubi N, Noroozi Pesyan N, Fathi M, Omidi Y. Injectable thermosensitive hybrid hydrogel containing graphene oxide and chitosan as dental pulp stem cells scaffold for bone tissue engineering. Int J Biol Macromol 2020; 162:1338-57. doi: 10.1016/j.ijbiomac.2020.06.138 [Crossref] [ Google Scholar]
- French A, Suh JY, Suh CY, Rubin L, Barker R, Bure K. Global strategic partnerships in regenerative medicine. Trends Biotechnol 2014; 32:436-40. doi: 10.1016/j.tibtech.2014.05.007 [Crossref] [ Google Scholar]