Bioimpacts. 16:32751.
doi: 10.34172/bi.32751
Review
Three-dimensional bioprinted hydrogels for the management of diabetic wounds: A review
Piyali Khamkat Data curation, Investigation, Methodology, Resources, Writing – original draft, 1 
Bramhajit Chatterjee Data curation, Investigation, Methodology, Resources, Writing – original draft, 1
Sourav Ghosh Data curation, Investigation, Methodology, Resources, 2
Bhupendra Prajapati Formal analysis, Visualization, 3
Biswajit Basu Formal analysis, Project administration, Visualization, 2, *
Sudarshan SIngh Conceptualization, Supervision, Validation, Writing – review & editing, 4, 5, *
Author information:
1Department of Pharmaceutical Technology, Brainware University, 398, Ramkrishnapur Road, Barasat, Kolkata 700125, India
2Department of Pharmaceutical Technology, School of Health & Medical Sciences, Adamas University, Barasat, Kolkata, West Bengal 700126, India
3Department of Pharmaceutics, Parul Institute of Pharmacy, Faculty of Pharmacy, Parul University, Waghodia, Vadodara 391760, Gujarat, India
4Office of Research Administration, Chiang Mai University, Chiang Mai, 50200, Thailand
5Faculty of Pharmacy, Chiang Mai University, Chiang Mai, 50200, Thailand
Abstract
Globally, the prevalence of diabetes mellitus (DM), a chronic metabolic disease, is at its peak. Type 2 diabetes (T2D) is more common worldwide, which raises the risk of ulcers and chronic healing, or non-healing wounds. Overall 15% to 20% of people with diabetes develop diabetic foot ulcers (DFUs), which is a significant consequence. Managing and treatment of wounds require an advancement of novel healing therapies with the use of biological dressings. The development of DFU wound dressings and the biomanufacturing of composite 3D skin substitutes are examples of 3D bioprinting technology for enhancing therapeutic approaches. These approaches and challenges of bioprinting technology in wound healing of chronic DFUs are covered in this review. Moreover, the review highlights the selection of biomaterials, integration of biomimetic approaches, and the ability of 3D bioprinting to replicate native skin architecture. Despite significant advances, the review identifies critical gaps including limited vascularization in printed constructs, standardization issues, and scalability challenges that impede clinical translation. Emerging biotechnological tools and novel biomaterial developments are also discussed, emphasizing their potential to overcome these limitations and improve DFU wound management.
Graphical Abstract
Keywords: Diabetes mellitus, Diabetic foot ulcers, Healing mechanisms, 3D bioprinting, Biomaterials
Copyright and License Information
© 2026 The Author(s).
This work is published by BioImpacts as an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/). Non-commercial uses of the work are permitted, provided the original work is properly cited.
Funding Statement
This research received no external funding.
Introduction
The largest organ of the human body, the skin, is prone to damage and may be responsible for $18.7 billion of the worldwide wound therapy market by 2027. The prevalence of diabetes mellitus (DM), a chronic metabolic condition, is rising worldwide. Persistent hyperglycemia and a deterioration in organ system function are its common characteristics.1,2 Diabetic foot ulcers (DFUs) are prevalent complications that negatively impact diabetes patients' overall quality of life.3,4 There can be a serious delayed wound healing of DFU patients due to their high sugar level in blood.5,6 Advanced dressings approaches are biocompatible, non-toxic, biodegradable and having ability to promote wound healing than traditional processes.7,8 In response, modern 3-dimensional (3D) bioprinting technologies have been designed to enhance wound care, especially in skin grafting operations and the fabrication of wound dressings.9,10 This technology can lower the expense of long-term healthcare systems and enable diabetic individuals to live healthier lives.11-14 Advances in 3D bioprinting, including better bioink formulations, increased precision, and vascular network integration, are covered in the article.
The skin is an essential organ that serves as a barrier between the body and its external environment. It weighs roughly six pounds and has a thickness of about 2 mm.15 The epidermis, dermis, and hypodermal are its three primary layers. The outermost layer, epidermis, is comprised of four sublayers that serve as a barrier to permeability. Fibroblasts, collagen, elastic fibres, blood arteries, nerves, and extracellular matrix are the dermis components that lie beneath it.16 The reticular and papillary layers consist of their two sublayers.17,18 The reticular layer is composed of blood vessels and the skin's appendages, whereas the papillary layer is comprised of dermal papillae that create a dermal-epidermal interface. The third major layer, the hypodermal layer, serves as an insulator for the tissues beneath it and shields the body from harm. Additionally, the skin contributes to the immune system, which shields us from illness.19 Out of all novel formulations, hydrogels are widely used for treating wounds due to their excellent moisture retention, biocompatibility, and ability to promote healing.20,21
DM causes DFUs, and the prevalence of DFUs is anticipated to increase as the population grows to 592 million by 2030. DFUs, the most serious type of diabetic sores, can cause lower limb amputation or even death and affect 15% of people with T2D. Eighty four percent of all lower limb amputations caused by diabetes are preceded by DFUs, emphasising the need to recognise ulcer pathogenic mechanisms. DFU is a type of wound that gets worse due to inadequate immune response, poor control of blood sugar, renal failure, and impaired vision.22 Diabetes patients' high glucose levels affect the functions of endothelial cells, keratinocytes, macrophages, fibroblasts, and delay wound healing.23,24 High glucose levels present an undesirable impact on re-epithelialization and inflammation resolution, resulting in chronic neutrophil and macrophage infiltration with an inability to resolve the inflammatory phase. Although endothelial cells are essential during the proliferative stage of healing, excessive glucose levels can prevent keratinocyte migration and angiogenesis, which reduces capillary density and vascularity. Not only that, but diabetes also raises the risk of ulcers, since it damages nerves, causes infection, and impairs circulation. The feet and legs are frequently affected by ulcers and the open wounds on the skin that don't heal properly.25 The Wagner Diabetic Foot Ulcer Grade Classification System is one of several grading schemes for diabetic ulcers. Cracks, dryness, redness, scaliness, and rash are some of the symptoms. A hard patch in the centre, discolouration, drainage, callosity, and an unpleasant odour are all possible symptoms of chronic ulcers.26 DFUs are common among diabetic elderly patients that indicate catastrophic effects, increasing the chance of amputation by up to 46 %. The risk of foot amputation can be decreased by the early identification of DFUs.27
Pressure ulcers, venous leg ulcers (VLUs), and DFUs are examples of chronic wounds that do not heal in three months due to well-controlled inflammatory phase. In chronic wounds, an imbalance between pro-inflammatory and anti-inflammatory cytokines leads to a delayed healing process.28 Additionally, wound infection increases inflammation and oxidative stress by impeding the transition from the inflammatory to the proliferative phases due to poor neutrophil function and decreased expression of innate anti-microbial peptides among DFU patients. By offering antimicrobial activity, drug delivery, scaffolds for tissue regeneration, and the maintenance of ideal wound conditions, biomaterials aid in DFU healing.3
Wound healing processes
The normal physiological process of wound healing involves mediators and cell interactions. Systemic problems such as dysregulated angiogenesis, chronic inflammation, neuropathy, hypoxia-induced oxidative stress, and affected neuropeptide signalling can be caused by diabetic hyperglycemia. Biological dressings and skin substitutes are two methods for treating diabetic wounds that emphasise lowering inflammation and utilising skin substitutes. Haemostasis, inflammation, proliferation, and remodelling are its four stages as presented in Fig. 1. Haemostasis is a process that keeps blood flowing and stops excessive bleeding. Whereas inflammation sterilises the wound and stops further infiltration. To coordinate the activity of neutrophils and monocytes towards the wounded location, tissue-resident macrophages release pro-inflammatory chemokines. Neutrophils undergo apoptosis, matrix metalloproteinases, and clearance to resolve inflammation. Collagen production and granulation tissue development occur during the proliferative phase. By transforming fibroblasts into myofibroblasts and breaking down the extra extracellular matrix and blood vessels, remodelling helps to restore the function and structure of the skin. The acute wound healing phase ends after dermal remodelling is achieved.
Haemostasis
Haemostasis is the first step in wound healing, during that process mast cell degranulation promotes bleeding and permits the infiltration of immune cells. The formation of a temporary scab occurs when the coagulation system is triggered. Examples of soluble mediators: a. growth factors like epidermal growth factor (EGF), vascular endothelial growth factor (VEGF), and platelet-derived growth factor (PDGF), b. danger-associated molecular patterns (DAMPs) like adenosine 5-triphosphate (ATP), histones, high mobility group box protein 1 (HMGB1), and genomic DNA, c. chemokines like CXCL-2 and IL-8 (CXCL-8), and d. Cytokines like IL-33, IL-25, and thymic stromal lymphopoietin (TSLP) are released by activated keratinocytes, fibroblasts, and platelets. These mediators serve as danger signals, causing patrolling inflammatory cells to infiltrate and local immune responses to be triggered.29,30
Inflammation
During the inflammatory phase of wound healing, extracellular matrix decomposition enzymes are released, inflammatory cells proliferate, and inflammatory mediators accumulate. In diabetic wounds, uncontrolled or extended inflammatory responses frequently result in poor wound healing or ulceration, whereas localised, well-regulated inflammation initiates proliferative and remodelling phases. A delay in wound healing process caused by neutrophil extracellular trap induction (NETosis), which is induced by T2D. Moreover, histone H4 and mitochondrial DNA cause more damage due to the ongoing activation of neutrophils and the development of NETosis. Additionally, during wound healing, skin-resident T-lymphocytes are crucial for preserving and controlling local skin inflammation. The healing rate is greatly decreased when regulatory T-cells (Tregs) are depleted. By promoting T-cell plasticity and Th17 cell differentiation towards T-regs, topical retinoic acid might accelerate the healing of diabetic wounds. Insufficiencies in anti-inflammatory cytokines produced by regulatory cells, such as M2 macrophages and T-regs, as well as elevated level of localised pro-inflammatory mediators are the causes of the prolonged inflammatory phase found in diabetic wounds, which slows healing and remodelling.31,32
Proliferation
Successful wound healing depends on the proliferative phase, which is highlighted by the development of proliferative tissue. Fibroblasts, immunological cells, and blood capillaries contribute to the migration of epithelial cells towards the wound surface during this phase. By releasing cytokines, growth factors, and chemotactic factors for stem and progenitor cells, these cells exhibit strong regenerative properties. However, skin-resident cell proliferation and activation are greatly decreased in chronic diabetic wounds. Reduced angiogenic capacity, oxidative stress, and T2D-mediated protein glycation are among the factors that cause the proliferative phase to unnecessarily prolong, leading to wound rupture. Additionally, significant cellular and molecular elements have been linked to wounds caused by T2D reported in previous literature.33
Remodelling
Endothelial growth factor (ECM) proteins develop scar tissue during wound remodelling, and M2 macrophages, myofibroblasts, and wound-resident fibroblasts are important components in this mechanism. The outcome of the scar is determined by the continual re-organisation of collagens, which comprise 85% of the dermis, during wound healing. Collagen fibres become thicker, denser, and more entangled as a result of the deposition and extraction of ECM components controlled by secreted matrix metalloproteinases and their inhibitors (TIMPs). Throughout the remodelling phase, the ECM is dynamically subjected to continual modifications, and skin restoration depends critically on its composition. It has been demonstrated that delivering ECM components of decellularized skin structures during wound healing enhances the healing process and has emerged as a promising treatment strategy. However, abolished angiogenesis causes oxidative stress and a hypoxic wound environment in wounds caused by T2D. Moreover, wounds treated with ECM components have shown increased and regulated fibroblast activity.32,33
Complications associated with diabetic wounds
DFUs are one of the familiar non-traumatic wounds in the lower limbs of the body. Skin redness and swelling are the first symptoms. If the wound is not treated, diabetes-related infections of the skin, bones, and tendons may develop, resulting in deeper sores. Charcot foot, claw feet, and hammertoes are examples of foot deformities caused by the degeneration of muscles and bones initiated by long-term diabetes. An infection in the wound causes abscess that might make it challenging to wear anything in leg.21,34 Therefore, if the wound is not treated instantly, it may result in partial or total gangrene, which can lead to the entire foot's skin tissues dying. Moreover, if the infection spreads to the tendons or bones, an instant therapy required to avoid sepsis, which can result in necrotising fasciitis (also known as flesh-eating disease).
Precise management of diabetic wounds through 3D printed hydrogels
Skin substitutes can be divided into groups according to their distinct compositions and derivative sources. Implantable scaffolds can be categorised by host origin, biomaterials from biologic sources, totally synthetic materials, acellular or non-acellular components, and dermal and/or epidermal components. To address the complexities of chronic wound conditions and individual clinical heterogeneity, successful skin substitutes frequently include a range of materials acquired from different sources. Due to their clinical results, safety, therapeutic effects, and ubiquity in DFU treatment, fully acellular dermal matrices are especially helpful.35 Three decades ago, 3D printing had an impact on several areas by offering the ability to develop a wide range of shapes and models quickly and affordably. Spritam (Levetiracetam), the first medication made by a 3D printer, achieved FDA approval in 2015 and is being marketed by Aprecia Pharmaceuticals.36 3D printing is flexible and adaptable method, offers resources for developing customised, individual therapies with efficient delivery systems. There are three types of 3D printing technologies: extrusion, inkjet, and laser solutions. It is crucial to consider the printer's resolution, biocompatibility, temperature, nozzle output volume, and affordability when selecting a 3D printer.33 The skin bioprinting process involves four steps: preprocessing (A), printing (B), postprocessing (C), and evaluation (D) (Fig. 2). Pre-processing involves selecting appropriate cell and ink bioprinting materials and designing the printing process. Postprocessing involves layering cell-laden bioinks, induced by epidermal keratinocyte differentiation and dermal fibroblast proliferation. Key indicators like sustained dermal cell viability and extracellular matrix production are considered before applications.37
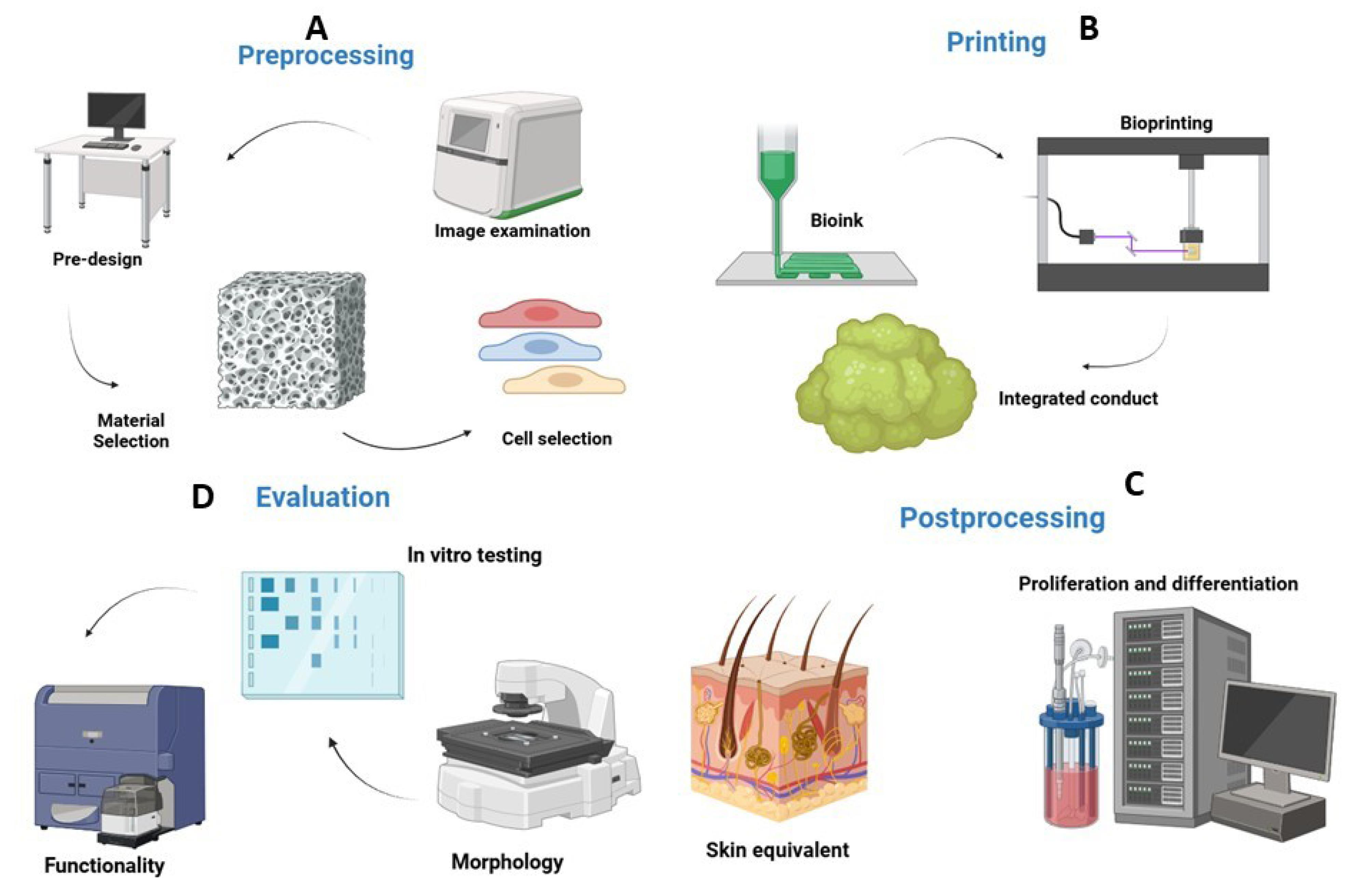
Fig. 2.
Steps involved for bioprinting of hydrogel with preprocessing (A), printing (B), postprocessing (C), and evaluation (D). Created in BioRender. https://BioRender.com/ytrcorm.
.
Steps involved for bioprinting of hydrogel with preprocessing (A), printing (B), postprocessing (C), and evaluation (D). Created in BioRender. https://BioRender.com/ytrcorm.
3D printing technique can assist diabetes patients in living better lives and distinguish DFUs from other chronic wounds.38 The fabrication of scaffolds for wound healing has been investigated using 3D bioprinting in recent years.39 For wound-healing applications, Glover et al designed 3D bio printed polycaprolactone (PCL) scaffolds loaded levofloxacin and studied their sustained drug release profile. The scaffold was designed for possible treatment of DFU and can be adjusted based on the size of the wounds. Compared to traditional therapy methods, this method is easier to use and less expensive according to the patient's needs.11
Comparison between conventional and advanced wound dressing
Millions of individuals throughout the world struggle with wound healing, and if left untreated, it leads to chronic infections. Conventional methods of wound protection, such as bandages, plasters, cotton, and gauze, may delay the healing process. However, due to different kinds of wounds and no specific dressing works for all of them, it is difficult to identify the most effective one. Current therapies such as lipid-based systems,40 synthetic and natural polymeric systems,41 emulgels, silicon microparticles, gold nanoparticles,42 and silver nanoparticles43 are some examples of novel drug delivery system. By delivering bioactive substances in a regulated and customised manner, 3D printed dressings may achieve the maximum therapeutic effects.23,33
Additive manufacturing technology
Rapid prototyping, also referred to as additive manufacturing (AM), or 3D printing, first appeared in the 1980s and has subsequently transformed several sectors, including biomedical engineering.44 AM enables precise, layer-by-layer fabrication, which facilitates the development of complex geometries and customized designs, in contrast to conventional manufacturing techniques that involve material removal or moulding.10 According to the American Society for Testing and Materials ASTM categorization, AM processes are classified into seven categories: binder jetting (BJ), material jetting (MJ), directed energy deposition (DED), sheet lamination (SL), material extrusion (ME), powder bed fusion (PBF), and vat photopolymerization (VP).45,46 Moreover, the potential techniques (Fig. 3) include droplet-based bioprinting, stereolithographic (SLA) printing, selective laser sintering (SLS), fused deposition modelling (FDM), and micro-extrusion bioprinting made the AM flexible in health applications, especially for managing diabetic wounds, is increased by the fact that each of these methods uses different material processing principles.47 Additionally, the capacity to customize polymeric structures with regulated porosity, mechanical characteristics, and bioactive functions has established AM (Fig. 4) as a pivotal technique for creating enhanced wound healing platforms, such as biocompatible hydrogels,48 drug-embedded films, and tissue-engineered dressings.49,50
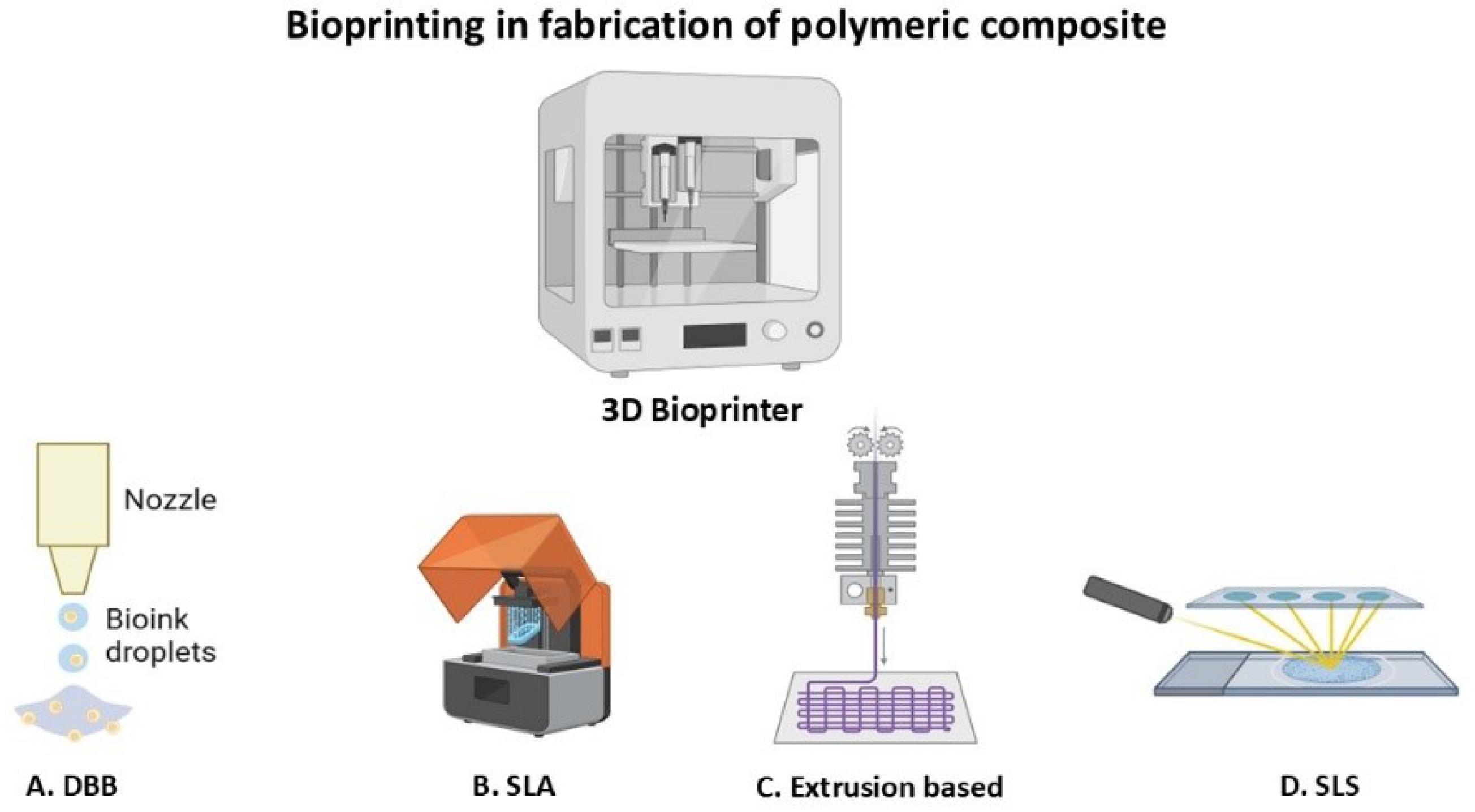
Fig. 3.
Potential bioprinting techniques, A. Droplet based bioprinting (DBB), B. Stereolithographic printing (SLA), C. Extrusion based bioprinting, D. Selective laser sintering (SLS). Created in BioRender. https://BioRender.com/ytrcorm.
.
Potential bioprinting techniques, A. Droplet based bioprinting (DBB), B. Stereolithographic printing (SLA), C. Extrusion based bioprinting, D. Selective laser sintering (SLS). Created in BioRender. https://BioRender.com/ytrcorm.
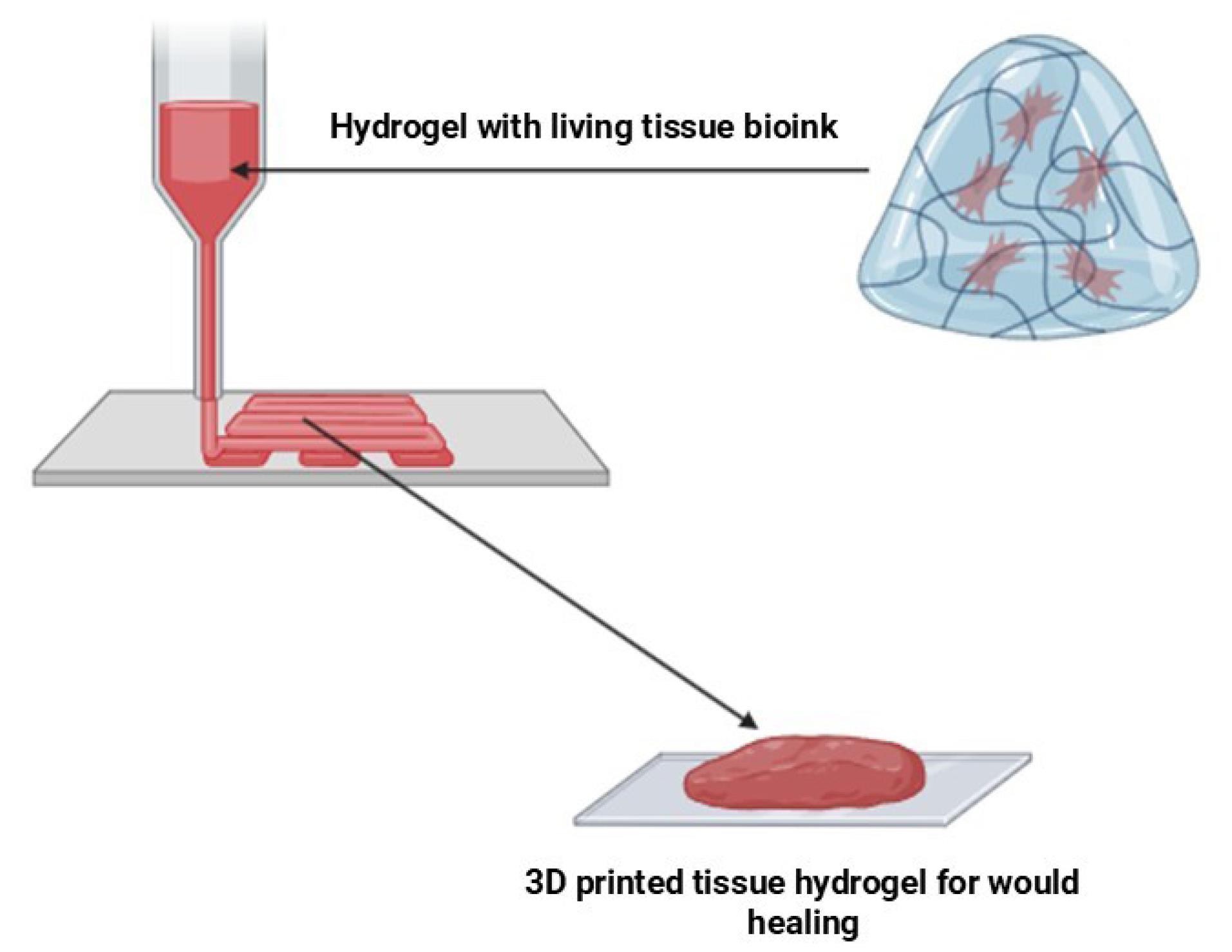
Fig. 4.
3D bio-printed polymeric tissue hydrogel with living cells for the tissue replacement in wound healing. Created in BioRender. https://BioRender.com/ytrcorm.
.
3D bio-printed polymeric tissue hydrogel with living cells for the tissue replacement in wound healing. Created in BioRender. https://BioRender.com/ytrcorm.
Droplet-based bioprinting
3D bioprinting seeks to develop tissue and organ structures by methodically depositing biologics, including living cells, biomaterials, pharmaceuticals, growth hormones, and DNA, in a sequential layer-by-layer manner.51 It allows for the development of tissue and organ constructions that are either scaffold-based or scaffold-free.52 The idea behind droplet-based bioprinting (DBB) comes from inkjet printing, which got its first product in 1951 when Elmqvist of Siemens invented the first useful inkjet device. Later, in 2000, Object Geometries developed the first 3D printer that used inkjet technology. In 2003, Boland established the viability of employing an improved thermal DOD inkjet printer for printing living cells in a functional state and proposed the idea of inkjet bioprinting.53 DBB provides high precision and adaptability in the fabrication of cell-laden scaffolds for biomedical applications.54 DBB, encompassing inkjet, acoustic, and micro-valve bioprinting, facilitates the precise deposition of bioinks containing living cells, biomaterials, and pharmaceuticals. It has significant limitations, compared to extrusion-based and laser-assisted bioprinting due to challenges such as nozzle clogging, a limited viscosity range of bioinks, and cell viability problems caused by mechanical or thermal stressors limit its widespread use in the fabrication of large, structurally stable structures.55 Moreover, SLA and SLS are advanced AM methods that utilize a laser to fuse powder particles or cure liquid resins, resulting in more precise construction of complex polymeric materials. DBB-based product has low mechanical strength, limited material viscosity, and problems building load-bearing structures, which makes it less useful for diabetic wound healing.56
Precise management of diabetic wounds through 3D printed hydrogels
Skin substitutes can be divided into groups according to their distinct compositions and derivative sources. Implantable scaffolds can be categorised by host origin, biomaterials from biologic sources, totally synthetic materials, acellular or non-acellular components, and dermal or epidermal components. To address the complexities of chronic wound conditions and individual clinical heterogeneity, successful skin substitutes frequently include a range of materials acquired from different sources. Due to their clinical results, safety, therapeutic effects, and ubiquity in DFU treatment, fully acellular dermal matrices are especially helpful.35
Stereolithography
Stereolithography (SLA) relies on the solidification of liquid resin through photopolymerization facilitated by ultraviolet (UV) light. In this procedure, the laser focus strikes a specific depth on the material's surface (liquid photo-polymerizable resins), solidifying the area it covers through photopolymerization.37 Biomaterial scaffolds are essential in tissue engineering (TE) and reconstructive medicine. Fundamental TE criteria for scaffolds encompass biocompatibility, biodegradability, and appropriate mechanical stiffness, which collectively facilitate cell and tissue development, integration, and remodelling.57 The most promising modelling method is solid free form fabrication (SFF), which offers the most precise control over the geometry of scaffolds using computer-aided design (CAD)-generated 3D models or clinical images.58 SLA is a highly promising fabrication technique, capable of producing objects with an accuracy of 20 microns.59 Currently, SLA fabrication technologies comprise two primary types: projection stereolithography (PSL) and laser stereolithography (LSL). When compared to LSL, which scans with a laser point-by-point, PSL builds an entire layer with just one shot, which greatly cuts the fabrication time.60 PSL is a prospective method due to its CAD capabilities, high fabrication speed, and fine resolution.61 PSL, utilizing digital light processors (DLP) and projectors, is garnering heightened interest due to its superior production speed and resolution. These qualities are achieved by projecting a complete image using masked illumination into the monomer solution, thereby simultaneously forming an entire layer and significantly decreasing manufacturing time.59 In diabetic wound care, scaffolds and polymeric hydrogels based on SLA offer enormous promise since they offer a customized, bioengineered method that replicates the natural ECM, promotes cell proliferation, and speeds up wound closure. In addition to providing structural support, these scaffolds encourage cell adhesion, proliferation, and differentiation all of which are essential for efficient wound healing.62 Furthermore, it has been demonstrated that adding growth factors to these scaffolds improves tissue remodelling and fibroblast proliferation, accelerating the healing of diabetic wounds.63
Fused deposition
The efficient recovery of DFU depends on a complicated process necessitating various combined therapeutic techniques in the treatment plan. Previously, FDM techniques for 3D printing were applied in a study of drug-loaded scaffolds for the treatment of DFUs.11 FDM has been investigated extensively in diabetic wound healing for developing bioengineered scaffolds and drug-loaded wound dressings, therefore offering structural support, controlled drug release, and tailored degradation rates to accelerate the healing process. Incorporating reinforcing elements such as hydroxyapatite,64 graphene, bioactive nanoparticles, and natural polymers65 has recently reported improving the biocompatibility, antibacterial characteristics, and mechanical strength of FDM-printed scaffolds.52 In contrast, to methods such as SLA and SLS, FDM has important drawbacks. FDM-printed items frequently show anisotropic mechanical properties, poor interlayer adhesion, and surface roughness due to their extrusion-based method, which may affect scaffold integrity and cell growth.66 Furthermore, FDM is not as precise and has lower resolution, compared to SLA. This makes it less ideal for creating complex microporous structures needed for cells to interact optimally in wound healing applications.67 Despite these obstacles, the potential of FDM in biomedical applications is being enhanced by ongoing process optimizations and material innovations, particularly in the production of personalized wound dressings and tissue-engineered scaffolds.68
Selective laser sintering
Selective laser sintering (SLS) is one type of AM that has a lot of benefits. For example, the printed parts are relatively strong, the unbonded powder can be recycled, and large batches can be printed without the need for support structures.69 Among the several areas, including medicinal, aerospace, automotive, and defence, SLS finds extensive application.70 SLS technology has various uses in medical engineering, such as the development of living prototypes for interventions, models for medical devices, and scaffolds for TE. SLS 3D printers are favoured in product development for their economic efficiency, elevated productivity, and diverse material compatibility. Advances in equipment, supplies, and technology have rendered SLS printing more widely available to a greater number of companies. FDM is frequently utilized in production; nevertheless, due to its constraints in producing complicated geometries, SLS is advised for sophisticated insole designs for diabetic foot.71 SLS provides exceptional precision, facilitating the fabrication of sophisticated insole structures with robust mechanical strength and complex geometries that improve pressure distribution and foot support. This method employs a laser to selectively sinter polymer powders, obviating the necessity for support structures and guaranteeing consistent mechanical qualities, which is essential for diabetic foot orthoses.72 Moreover, SLS facilitates the integration of sophisticated porous configurations, including triply periodic minimal surface structures, which enhance flexibility, breathability, and overall patient comfort. Materials appropriate for SLS-printed insoles can be customized for certain mechanical qualities, enhancing offloading and diminishing plantar pressure in diabetic individuals.73 Before clinical application, SLS-manufactured insoles undergo stringent in silico and in vitro assessments to determine their pressure-relieving efficacy.74 Future research is to incorporate flexible sensors for real-time foot monitoring, optimize topology for lightweight structures, and apply machine learning for inverse design, thereby enhancing the efficacy of DFU control strategies.75
Extrusion-based bioprinting
Extrusion-based bioprinting can generate 3D scaffolds from biomaterials and living cells to heal damaged tissue and restore function. Extrusion-based bioprinting has transformed from a straightforward technique to one that can generate a diverse array of tissue scaffolds from a variety of biomaterials and cell types in the past two decades, as a result of advancements in both the engineering field and biological sciences.76 It successfully prints porous 3D structures using a variety of configurations, such as fibrous strands, filamentous elements, and beaded formations, all of which contribute to their structural stability and functionality. Furthermore, rolled layers, sheet-based structures, and grid-like frameworks offer fabrication flexibility, while interconnected channel networks improve permeability and fluid movement within these engineered systems, and they imitate tissue components at both micro and macro levels.77 Vasculature formation is a significant challenge in TE, supplying oxygen, nutrients, and metabolites for long-term cell and tissue viability. Extrusion-based bioprinting uses vessel-like channels to facilitate vascularization, with endothelial cells deposited to initiate vasculature formation.78 Extrusion-based technologies are particularly beneficial for printing high-viscosity materials like PCL, which is FDA-approved and biocompatible. PCL is used for scaffold creation in bone and tissue regeneration, providing a robust supporting structure for wound healing.79 Diabetes-related wound-healing issues can be exacerbated by factors like diabetic neuropathy and peripheral arterial disease. To address this, Levofloxacin (LFX), a fluoroquinolone antibiotic, was used in a bioprinting study to create LFX-loaded PCL scaffolds.80 The scaffolds were tested against pathogenic bacterial strains in the context of DFU. The 3.0 % LFX scaffold demonstrated the longest duration of release, indicating its suitability for sustained drug delivery.81 The scaffold design demonstrated suitable mechanical properties for TE and can be easily modified to the wound size. This study provides a low-cost alternative to current DFU treatments, demonstrating the potential of bioprinting in wound healing.11 Extrusion-based bioprinting offers a novel method for diabetic wound healing. This technology combines biocompatible scaffolds with antibiotic delivery to provide infection control, mechanical support, and long-term healing effects. Future enhancements could incorporate multi-layered scaffolds containing additional bioactive compounds to increase treatment effects.82
3D DFUs Models for Bioprinting
The mouse model is generally employed in 3D printing due to its wound healing mimicking property of that the human body. Organotypic 3D printed skin models may promote wound healing through stimulating angiogenesis or regeneration, decreasing inflammation, or preventing fibrosis. These models can be classified as scaffold or scaffold-free systems. As scaffolds change porosity, surface, and permeability, are frequently utilised. 3D human skin equivalent models and other hyperglycaemic wound models have been used to research of diabetic inflammation. The 3D endothelial cell germination test can be utilised as a screening tool for hyperglycaemic applications and is more representative of the angiogenic process of endothelial cells than the conventional 2D test. 3D printing allows for great customisation, quick creation of complicated structures (Fig. 5), with better flexibility and accuracy of in vitro models.39,83
Bioinks
Bioinks are substances that possess biological and physico-mechanical characteristics with the targeted tissues. Depending on the printer and target tissue, they can be altered and must be printable. Because of their high mechanical and functional requirements as well as their biocompatibility, multicomponent bioinks are preferable to single-component bioinks. Natural substances including collagen, fibrin, alginate, and gelatin are utilised extensively as biomaterials due to their nontoxic and biocompatibility property. Natural materials have also been supplemented with synthetic polymers such as polyurethane, poly(lactic-co-glycolic acids), polyethylene glycol, and PCL.33
Agarose, an organic polysaccharide derived from red seaweed, is widely used as bioink due to its thermo-reversible gelling action and biocompatibility. Brown algae produce alginate, an anionic polymer, which can form hydrogels with properties similar to the extracellular matrix of tissues. In bioinks, cellulose, a stiff polymer, can be added in altered content to increase its porosity, strength, and flexibility. Nanocrystals of carboxymethyl cellulose can improve shear-thinning behaviour and mechanical strength. Collagen and chitosan can also be used as bioinks.84,85 Biodegradable scaffolds can be made by chemically modification of dextran,86 a nontoxic, hydrophilic homopolysaccharide. Blood contains a soluble protein called fibrin, which is utilized to make different tissues. Because of its rapid gelation and high initial stability, gelatin, a thermosensitive polymer, is utilized as an element in bioink. Gellan gum is a biocompatible and biodegradable polymer that is utilised in bioprinting. Although HA is a biocompatible, biodegradable, and bioresorbable substance that aids in wound healing and has potential applications in bioprinting, it necessitates crosslinking.87 Though biological inks frequently contain regulatory elements like cytokines and chemokines, it is challenging to replicate intricate microenvironments and intercellular interactions. Because of its extraordinary biocompatibility, printability, and preserved partial ECM structure, decellularized extracellular matrix (dECM) has emerged as a new bioink option for skin bioprinting. Although it is still difficult to remove heterologous dECM's immunogenicity while maintaining its structure and biological activities. Exosomes and platelet-rich plasma are two examples of naturally occurring microenvironmental factor combinations that have drawn interest in bioprinting.88,89
Technical aspects of hydrogel in 3D printing
Before and after printing, the following evaluations can be performed to check the quality of the hydrogels used in 3D printing.
Rheology
Polymers are both elastic and viscous, and the complex shear modulus (G*) describes their viscoelastic response. The frequency sweep test can be used to determine the time and frequency dependence of viscoelasticity in polymers. The formula 𝐺∗ = 𝐺′ + 𝑖𝐺″ can be used to represent the complex shear modulus. G″ represents the loss modulus, and G′ represents the storage modulus.
Extrusion velocity
The Allevi 2, a pneumatic material extrusion 3D printer can be utilised to prepare samples and print materials. Temperatures and pressures must be adjusted by the printer from room temperature to 140 °C and 6.90-827 kPa respectively. An EOS REBEL T3i DSLR camera is used to record the extrusion after a complete metal nozzle with a 450 µm in diameter. The recordings are then turned into pictures to determine the extrusion velocity. The printed strut is then implemented to measure the strut diameter after the materials are placed on a substrate with a layer height of 450 µm.90
Precise management of diabetic wounds through 3D printed hydrogels
The printability of a 3D bioprinter can be modified by FDM using cellulose and gelatin salts. Because of its superior printing properties, polymers like Pluronic can be employed as a control bioink. For best results, basic line patterns are required to be printed following G-codes and printer settings. Printability evaluation is essential for assessing the quality of bioink.91
Strut Diameter
Using SOLIDWORKS 2021, a cylindrical sample with an open porosity can be examined. Slic3r is used to slice the 3D model after the STL file creation. 3D printing was done using the G-code file.90
Degradation evaluation
By exposing the materials to four degrading effects temperature, humidity, UV light, and winter weather the study is examined to verify the mechanical properties of the materials. The samples are exposed to furnace settings, temperature cycling, UV light, and a condensation chamber. According to a recent finding, the samples' surfaces become slightly sticky and yellowed after being exposed to UV light. Additionally, the samples are performed 98 days of outdoor ageing in conditions that vary in temperature, sunshine, and air humidity.92
Applications of 3D printed hydrogels in management of diabetic wounds
Hu et al investigated the impact of hyperglycemia on vascular endothelial cells (HUVECs) and suggested that Bone Marrow Mesenchymal Stem Cell derived exosomes can reduce the dysfunction. Researchers developed a 3D scaffold dressing composed of mesoporous bioactive glass (MBG) and decellularized small intestinal submucosa. This SIS/MBG@Exos hydrogel showed an improvement in HUVEC activity and angiogenesis in diabetes induced Sprague-Dawley (SD) rats. The study was performed for 14 days and proved that the hydrogel accelerated diabetic wound healing, enhanced blood perfusion, and promoted collagen deposition93 (Fig. 6). Lin et al prepared 3D-printed porous hydrogel scaffolds using bio-inks such as gelatin (Gel), sodium alginate (SA), CaCO₃ microspheres, and oxidized sodium alginate (OSA) to promote wound healing. The SA/OSA/Gel scaffold demonstrated superior structural stability and accelerated NIH-3T3 cell growth. These scaffolds demonstrated 93.0 ± 2.5% collagen deposition between broken fragments, expedited wound healing, and encouraged angiogenesis when applied on SD rats for 14 days.94 An artificial intelligence (AI)-assisted high-throughput printing-condition-screening system was demonstrated to maximize 3D bio-printing conditions for hydrogel structures by Chen et al. The system offered satisfactory mechanical properties, biological performances in vitro, and the ability to speed up diabetic wound healing by performing an animal study.95
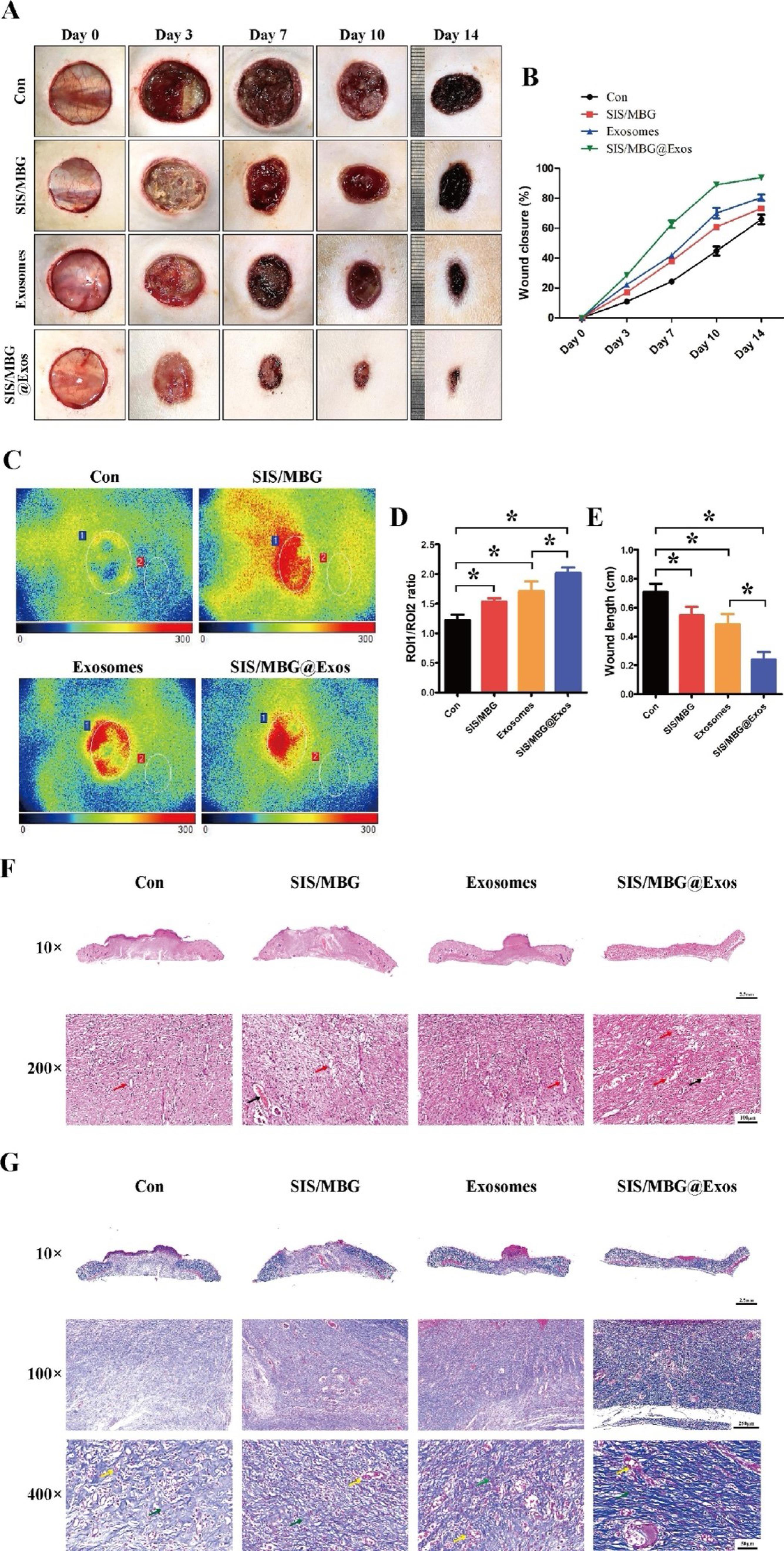
Fig. 6.
3D printed hydrogel scaffolds promoted diabetic wound healing. Effects on wound healing on day 0, 3, 7, 10 and 14 post-surgeries (A). The rate of wound closure among the different groups was calculated using the ImageJ software (B). Blood perfusion of the wound was assessed using doppler detection. Perfusion is presented as the ratio of wound area (ROI-1) to area surrounding the wound (ROI-2) (C, D). H&E staining and quantification of wound length of the four groups, Scale bar:2.5 mm and 100 μm (E, F). Masson’s staining of the wound bed of the four different groups, Scale bar:2.5 mm, 250 μm and 50 μm(G). Reprinted from Lozano et al84 Copyright (2026), with permission from Elsevier.
.
3D printed hydrogel scaffolds promoted diabetic wound healing. Effects on wound healing on day 0, 3, 7, 10 and 14 post-surgeries (A). The rate of wound closure among the different groups was calculated using the ImageJ software (B). Blood perfusion of the wound was assessed using doppler detection. Perfusion is presented as the ratio of wound area (ROI-1) to area surrounding the wound (ROI-2) (C, D). H&E staining and quantification of wound length of the four groups, Scale bar:2.5 mm and 100 μm (E, F). Masson’s staining of the wound bed of the four different groups, Scale bar:2.5 mm, 250 μm and 50 μm(G). Reprinted from Lozano et al84 Copyright (2026), with permission from Elsevier.
AI and 3D printing technologies have increased material compatibility and accuracy used for diabetes wound therapy. For machine learning-based wound dressings, functional 3D-printing inks were fabricated using DNA derived from salmon sperm and DNA-induced bio silica modelled after marine sponges by Kim et al. As per the study, these inks offered better mechanical tunability, porosity, and efficient blood absorption, accelerated anti-inflammatory potential for rapid wound healing on animal models for 15 days.96 Li et al designed a new hydrogel ink based on chitosan for the quick in situ development of customized diabetic wound dressings. Because of this ink's self-supporting qualities, high-fidelity 3D printing is possible without the need for extra processing and it has shown biodegradable, mechanical, antimicrobial, anti-swelling, and pro-angiogenic qualities applied on mice for 17 days.97 To help diabetes patients with persistent wounds, a new multifunctional bilayer wound dressing composed of PCL, cellulose acetate (CA), sodium alginate, gelatin, polyvinyl alcohol, and hyaluronic acid was developed by Rahman Gamal et al. PCL/CA2/LSGPH dressing showed strong antibacterial and anti-inflammatory qualities. Research has proven that it inhibited S. aureus and E. coli, speed up wound healing, and promoted re-epithelialization, collagen deposition, and neovascularization when applied on 30 male rats for 14 days.98 Aloe vera gel and bovine serum albumin combination was developed to produce a novel amyloid-based hydrogel by Naik et al. The effectiveness of the hydrogel in speeding up chronic wound healing was examined using diabetic Wistar rats for 21 days, and its in vitro wound healing properties were assessed using 3T3 fibroblast cells.99
For diabetic wound healing, a 3D-printed hydrogel made of deferoxamine, oxidized mannan oligosaccharide, and acrylamide based on hyaluronic acid (HA-AM) has been generated by Yang et al. Diabetic wound healing is hampered by chronic inflammation. By efficiently controlling RAW264.7 macrophages and encouraging M2 polarization, HA-AM/OMOS@DFO hydrogel breaks down the barrier of inflammation applied on SD rats for 12 days.100 An egg white-based natural hydrogel was introduced for the treatment of diabetic chronic wounds by Guo et al. Without the need for exogenous growth factors, the 3D-printed egg white hydrogels with a secondary network can promote wound healing through proangiogenic effects with improved collagen deposition101 (Fig. 7). Cao et al designed 3D-printed conductive hydrogel strips of gelatin methacrylate (GelMA) and [2-(acryloyloxy) ethyl] Trimethylammonium chloride (Bio-IL) filled with doxycycline hydrochloride, which encouraged skin regeneration in diabetic wounds of SD rats for 21 days.102
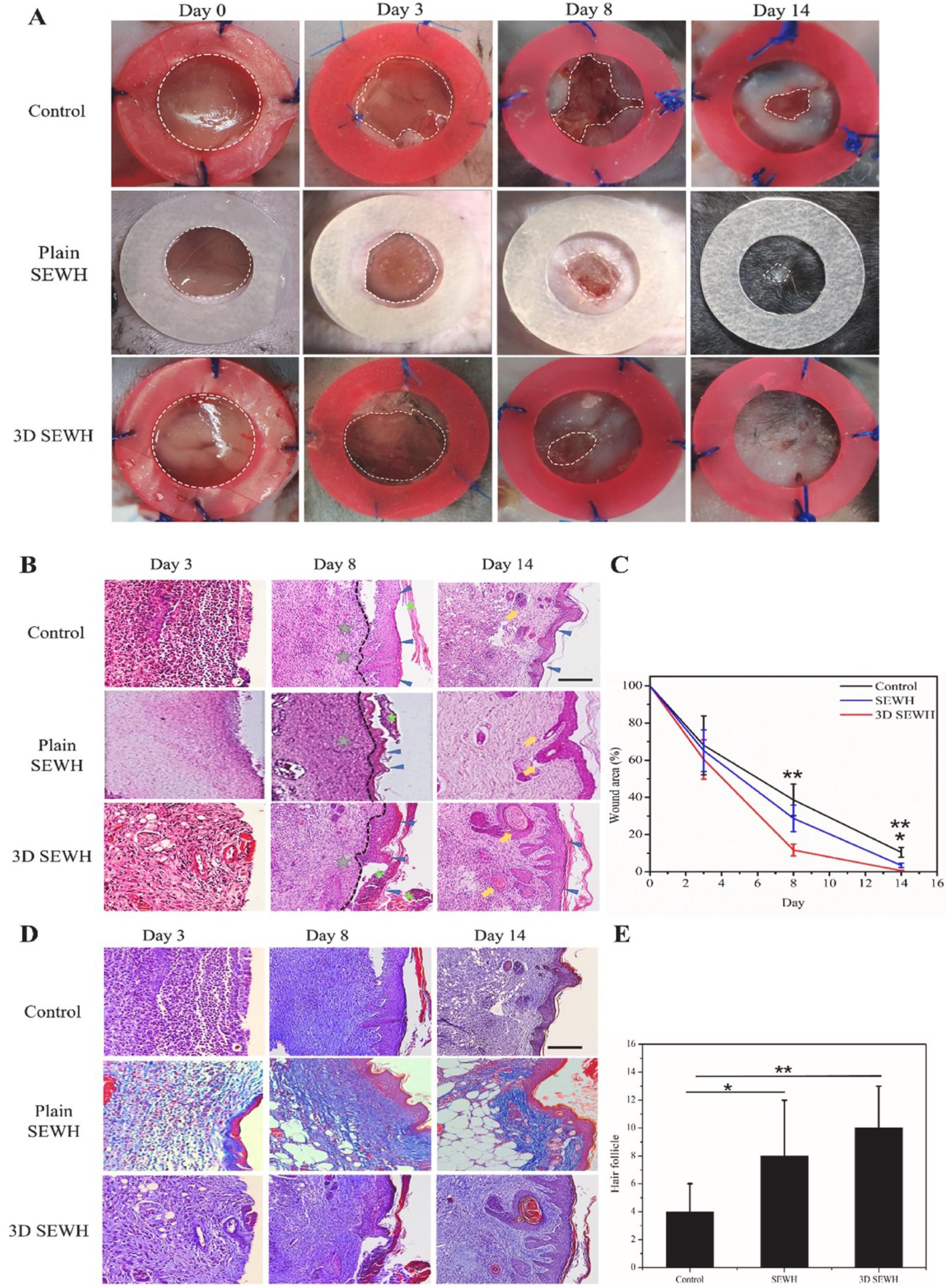
Fig. 7.
Macroscopic skin regeneration panorama with control, plain, and 3D SEWH group over 14 days, the inner diameter of ring silicone splint was 10 mm (A). H&E staining (scale bar = 100 μm) of healed wound skin (B), the quantification of wound closure (C) and MT staining (scale bar = 100 μm) (D). Quantification of hair follicle regeneration (E). Reprinted from Lin et al94 under Creative Commons CC-BY-NC-ND license.
.
Macroscopic skin regeneration panorama with control, plain, and 3D SEWH group over 14 days, the inner diameter of ring silicone splint was 10 mm (A). H&E staining (scale bar = 100 μm) of healed wound skin (B), the quantification of wound closure (C) and MT staining (scale bar = 100 μm) (D). Quantification of hair follicle regeneration (E). Reprinted from Lin et al94 under Creative Commons CC-BY-NC-ND license.
Using in situ 3D bioprinting, the work introduces a MoS2-accelerated gelling hydrogel scaffold for the healing of chronic diabetic wounds was prepared by Ding et al. It was created by combining MoS2 nanosheets with dextran solutions functionalized with benzaldehyde and cyanoacetate groups to reduce oxidative stress, encourage closure, speed up wound healing, and get rid of bacterial infections in a group of diabetes mouse models for 15 days.103 Liu et al designed a combination of polymerizable deep eutectic solvent solution (PDES) and a recyclable eutectogel backing layer in a 3D-printed dissolving microneedles (DMN) patch. In diabetic rats, the researchers demonstrated the effectiveness of their ternary PDES for a needle part, which combines biocompatible choline chloride, itaconic acid, and N-vinyl-2-pyrrolidone for effective drug administration and controlled glucose release. According to the study, the combination of DMNs with adhesive backing dramatically expedited the healing process, and by day 10, the CHPG-TA@CUR treatment group had a considerably greater wound healing rate (68.08 %).104 Lihao et al developed a new porous scaffold with sodium alginate, gelatin, and salvianolic acid B using 3D bioprinting technology. In rat model, the scaffolds exhibited potent anti-inflammatory, proangiogenic, rapid wound healing, and antioxidant qualities. The scaffold proved that it can promote the expression of transforming growth factor-β, decrease the expression of tumour necrosis factor, interleukin-6, and interluekin-1β, and eliminate reactive oxygen species applied on rats for 14 days.105 For wound healing, a hydrogel scaffold that has been 3D printed and loaded with natural Centella asiatica extract has been created by Wang et al. The research proved that bio-ink, such as gelatin and sodium alginate, may suit the contour of the wound, coordinate immunological responses and macrophages, and encourage healing when applied on Kunming (KM) mice for 7 days.106 In order to treat diabetic wounds, Hu et al. introduced a bio-printed dermal scaffold that used an EM-based hydrogel system loaded with copper epigallocatechallate (Cu-EGCG) capsules. The scaffold offered a rapid healing of diabetic wounds in rats for 7 days by promoting angiogenesis and lowering inflammation. Treatment of diabetic lesions, particularly foot ulcers, is difficult because of their intricate pathophysiology. It has been demonstrated that adding stem cells to curcumin-chitosan nanoparticles improves wound healing by Piva et al. StemCurCol scaffolds contributed to regeneration in mice with generated wounds by demonstrating improved re-epithelialization, faster closure rates, and faster wound closure.107 Using platelet-derived growth factor-BB (PDGF-BB) loaded 3D printed gelatine scaffold and silver-laden gelatine cryogel, Wan et al have created a bilayer skin substrate for diabetic wound healing. The scaffolds loaded with silver killed bacteria considerably and had no influence on cell proliferation. Silver and PDGF-BB coloaded scaffolds demonstrated potential for diabetic wound healing and bacterial infections in vivo by speeding wound closure, re-epithelialization, granulation tissue development, and angiogenesis.108
Clinical case studies
In vitro investigations have demonstrated the effectiveness and safety of 3D-printed materials in healing difficult wounds. To make sure their microstructure can stick to the wound site and replicate the microenvironment in a real scenario, 3D-printed items must be tested on humans. A clinical trial showed that 3D printing inks effectively healed fractures in both small and large bones due to their bio adhesiveness and biocompatibility. A 3D-printed PLLA and gelatin scaffold has been investigated for wound healing in persons over 18 years. The scaffold promotes re-epithelialization and wound closure, sticks to the wound, and rapidly develops a fibrin membrane. More case studies with a larger cohort and control group are required to evaluate the efficacy of 3D-printed wound healing products.33,83 Table 1 represents clinical trials of 3D Printing used in DFU treatment.
Table 1.
Clinical trials of 3D Printing used in DFU treatment
|
Treatment
|
Objective
|
Participants
|
Result
|
References
|
| 3D Printing |
To investigate the potency of autologous micro fragment adipose tissue injection in contrast to conventional therapy. |
114 |
Autologous micro-fragmented adipose tissue injected locally is a legitimate and safe treatment option that can speed up the healing process after minor amputations of irreversible DFUs. |
109
|
| To provide autologous minimally manipulated homologous adipose tissue (AMHAT) therapy to promote high-quality primary care. |
10 |
For individuals with chronic DFUs, bio printed AMHAT therapy was found to be a safe and successful treatment option. |
110
|
| To check the potency of 3D-printed manipulated extracellular matrix (MA-ECM) made from autologous homologous adipose tissue in DFUs. |
17 |
Wound healing is accelerated by MA-ECM-based therapy. |
111
|
| To ascertain whether 3D-bioprinted autologous adipose tissue grafts are effective on DFUs |
10 |
Using a 3D bioprinter for autologous adipose tissue grafting facilitated wound healing and provides superior skin repair. |
112
|
Advancement in 3D printed scaffold printing with cells for improved tissue engineering
There is a significant potential for the regeneration of intricate tissue structures or entire organs through the use of TE scaffolds. The fabrication of TE scaffolds, which possess an exceedingly intricate structure, is feasible and precise through the utilization of 3D printing techniques. Furthermore, they facilitate the application of computer-assisted approaches to TE scaffold design.113 Organoid technology provides a significant possibility to accurately replicate in vivo tissues by creating 3D structures.114 3D technology enhances skin tissue regeneration and wound healing in diabetic patients by precisely replicating the biological microenvironment, improving intercellular interactions and bio-signal transduction. This enables the cells that promote wound repair to exhibit increased levels of survival and differentiation.115 These scaffolds replicate the original extracellular matrix, enabling cellular adhesion, proliferation, and differentiation while also encouraging vascularization, which are the key aspects for effective tissue regeneration.11 Using bioinks that contain stem cells, growth factors, and antimicrobials has made printing scaffolds much better at helping wounds heal faster and restoring skin integrity.116 Smart scaffolds with controlled drug release mechanisms provide long-term therapeutic benefits, including reduced infection risks and increased cellular activity. Innovations in bio-fabrication techniques, such as extrusion-based and laser-assisted bioprinting, enable the precise spatial arrangement of different cell types, enhancing scaffold performance.117 Furthermore, hydrogels and biopolymers such as collagen, alginate,118 sericin,119 and fibrin are increasingly being employed to improve scaffold biocompatibility and mechanical stability, resulting in an ideal environment for skin regeneration.120 These engineered constructions show significant potential in managing the problems of chronic diabetic wounds by giving tailored and regenerative therapeutic methods, ultimately shortening healing time and increasing patient outcomes.121
Regulatory prospectus associated with 3D-printed scaffold printing
The popularity of 3D printing in drug manufacturing has grown dramatically since the COVID-19 epidemic, especially in the pharmaceutical and healthcare industries. Although the FDA offers recommendations on additive manufacturing, issues with quality control and intellectual property have come up. Because of their active characteristics, nanomaterials employed in additive manufacturing are challenging to evaluate and control. Additional data from the industry of these 3D printing materials is needed by regulatory bodies in the USA, Canada, and Europe. It will be difficult to put this technology on the market since regulatory bodies need to create efficient plans, rules, and regulations to regulate the production and use of printed pharmaceuticals. To assure patient safety, efficacy, and stability, 3D printed products must pass the same regulatory process. Standardising AM processes, encompassing hardware, software, testing protocols, inputs, quality parameters, environment, health and safety, foundations, and vocabularies, is the goal of ISO/TC 261. Under the FD&C Act, MDUFA, and Cures Act, the FDA governs 3D medical printing commodities. Class I, II, and III devices are categorised according to their level of risk. Guidelines on the technical, design, and content of 3D-printed medical devices have been released by the FDA. Technical Considerations for the Development and Evaluation of 3D-Printed Medical Devices, "Guidance for the Content and Format of Premarket Submissions for 3D-Printed Medical Devices," and "Recommendations for 3D Printing in the Development and Manufacturing of Medical Device Products" are a few of these.33,122
Challenges associated with 3D-printed scaffold printing
Because of unintended cellular interactions and stem cell differentiation, traditional 3D printing and tissue engineering materials are not biologically suitable. To replicate the flexible and nano-structural characteristics of the original tissue, novel hydrogels and biopolymers are being developed. These materials might lack the structural strength required for the best bioprinting outcomes. The existing method of bioprinting takes a long time and does not always produce the quantity of cells required for a variety of tissue types. Selecting the right bioink, managing shear stress, and maximising printing conditions and bioink uniformity are all crucial challenges in the process.
Vascularity is a crucial barrier in bioprinting because it allows tissues to grow and survive beyond the oxygen diffusion limit of 100–200 mm. Tissues may have physiological restrictions in the absence of a circulatory network, which could result in necrosis or incomplete tissue formation. Due to printing resolution and speed restrictions, bioprinting vasculature is currently facing difficulties. Creating artificial vascular networks or integrating angiogenic growth factors into bioinks are two ways of improving in vivo vascularization. However, the basic challenge of rapidly developing mature, functional vasculature to promote tissue development and avoid tissue death is still unresolved.123 Furthermore, the regulatory approval procedure may take longer due to the complexity of 3D-printed devices, and regulators may find it difficult to keep up with the rapid advancements in 3D printing technology. Significant obstacles include processing time and cost, but bioprinting may be more economical for customised products.124
Future aspects
Current 3D skin models have limitations due to the lack of elements such as immune cells, blood vessels, nerves, and sweat glands. Creating a unified bioink model of the skin is a major challenge. Topical treatment with dressings is used in DFU management practices (Fig. 8), but they are expensive and ineffective. To facilitate precise measurements, raise awareness of foot health, and encourage the prevention and treatment of foot issues, software quality must be improved. Customised footwear and dressings made with 3D printing technology can improve fit and protection, which is advantageous for improved DFU management.33 3D printer farms are a new approach to speed up large-scale production of mimic products. Thus, developing new biocompatible ECM-based hydrogels as bioinks is one strategy that can produce an ECM microenvironment in printed skin constructions that resembles the original one.125 Personalised treatment is another application for 3D bioprinting, which enables the size and shape of constructs to be altered to match the particular wound structure of each patient. Furthermore, bioactive compounds can be added to acellular 3D-printed wound dressings by 3D bioprinting, strengthening their antimicrobial and pro-healing qualities.23,126
4-D printing (4DP) uses stimulus-responsive materials and smart biomaterials to transform 3D-printed items into various configurations. Despite limitations in size reduction and folding simplicity, it has potential for developing new dosage forms and improved DDS for wound healing.127 3D printing technology has demonstrated potential to develop new dosage forms and improve DDS for the treatment of wound healing.128
In addition to forecasting infection risk or healing trajectories, AI and machine-learning algorithms provide benefits by automating wound assessment using photos and 3D scans. Based on past research results and patient characteristics, AI can suggest drug dosages, dressing designs, and reprinting intervals. According to clinical research, AI wound apps support clinical integration by measuring and classifying DFUs with good accuracy.103 The future proposals include (1) developing hydrogel-compatible, low-power, disposable biosensors; (2) developing standard datasets and AI models for wound segmentation; (3) combining cloud AI and smartphone 3D scanning to create customized dressings; and (4) performing early human studies to evaluate the effects on healing, patient adherence, and the economy. The practical use of smart, customized hydrogel dressings for diabetic wounds will be made faster by these endeavors.104
Conclusion
Stem cell-supported biological dressings, such as skin substitutes, might be a viable alternative of DFU treatment. Innovative approaches will be developed by additional research on biomaterials and skin substitute properties. Natural polymer-based hydrogels, particularly those derived from collagen, chitosan, alginate, and hyaluronic acid, are useful for treating diabetic wounds because of their capacity to deliver bioactive agents that promote the healing of DFUs, as well as their biocompatibility, biodegradability, and moisture retention. Though its application in wound healing has not received much attention, 3D printing technology provides customised treatment for DFUs. Developing 3D models, encouraging keratogenic cell development, and investigating wearable technology are some of the difficulties. Medical practitioners are also not well-informed on the use of 3D printing in the treatment of DFUs.
Review Highlights
-
3D Hydrogels are biocompatible materials effective for treating diabetic wounds by carrying drugs, promoting healing, and maintaining a moist environment.
-
This paper highlights the use of 3D printing to produce customized hydrogel dressings with enhanced mechanical strength, controlled and improved healing effectiveness.
Competing Interests
The authors declare no conflicts of interest.
Ethical Approval
Not applicable.
Acknowledgements
This work is partially supported by CMU Proactive Researcher Scheme (2023), Chiang Mai University for Sudarshan Singh.
References
- Mi W, Xia Y, Bian Y. The influence of ICAM1 rs5498 on diabetes mellitus risk: evidence from a meta-analysis. Inflamm Res 2019; 68:275-84. doi: 10.1007/s00011-019-01220-4 [Crossref] [ Google Scholar]
-
Patel M, Shah P, Singh S, Prajapati BG. An Insight on Flavonoids and Flavonoidsincorporated Nano-formulations in the Management of Diabetes Mellitus. Curr Diabetes Rev 2025. doi: 10.2174/0115733998354264250402054755.
- Tan CT, Liang K, Ngo ZH, Dube CT, Lim CY. Application of 3D bioprinting technologies to the management and treatment of diabetic foot ulcers. Biomedicines 2020; 8:441. doi: 10.3390/biomedicines8100441 [Crossref] [ Google Scholar]
-
Mistry PS, Singh S, Chorawala MR, Prajapati BG, Kapoor DU. Unlocking the Potential of Carrier Mediated Nano-biomedicine in Management of Diabetes Mellitus: A Review. Chem Biodivers 2025. 22: e202402258. doi: 10.1002/cbdv.202402258.
- Zhao M, Huang J, Yang H, Yang R, Guo S, Liu Z. Engineered aggregation-induced emission luminogens-based framework with CO-releasing property for accelerating diabetic wound healing. Chem Eng J 2025; 524:168981. doi: 10.1016/j.cej.2025.168981 [Crossref] [ Google Scholar]
-
Puri A, Mohite P, Singh S, Chaudhari Y, Chaudhari M, Ansari Y, et al. Biomaterials-Based Additive Manufactured Products for Diabetic Wound Healing. In: Singh S, P Mohite, D Datta, editors. Biomaterial-based Additive Manufacturing in Tissue Engineering and Regeneration. Cham: Springer Nature Switzerland; 2025. p. 279-312. doi: 10.1007/978-3-031-96070-3_10.
- Zhang Y, Nie C, Wang Z, Lan F, Wan L, Li A. A spatial confinement biological heterogeneous cascade nanozyme composite hydrogel combined with nitric oxide gas therapy for enhanced treatment of psoriasis and diabetic wound. Chem Eng J 2025; 507:160629. doi: 10.1016/j.cej.2025.160629 [Crossref] [ Google Scholar]
- Guo X, Li J, Wu Y, Xu L. Recent advancements in hydrogels as novel tissue engineering scaffolds for dental pulp regeneration. Int J Biol Macromol 2024; 264:130708. doi: 10.1016/j.ijbiomac.2024.130708 [Crossref] [ Google Scholar]
-
Xu Y, Zhang F, Zhai W, Cheng S, Li J, Wang Y. Unraveling of Advances in 3D-Printed Polymer-Based Bone Scaffolds. Polymers (Basel) 2022; 14. doi: 10.3390/polym14030566.
-
Wu Y, Chiu G, editors. An improved height difference based model of height profile for drop-on-demand 3D printing with UV curable ink 2021: IEEE. doi: 10.48550/arXiv.2409.07021.
- Glover K, Mathew E, Pitzanti G, Magee E, Lamprou DA. 3D bioprinted scaffolds for diabetic wound-healing applications. Drug Deliv Transl Res 2023; 13:2096-109. doi: 10.1007/s13346-022-01115-8 [Crossref] [ Google Scholar]
- Shi T, Lu H, Zhu J, Zhou X, He C, Li F. Naturally derived dual dynamic crosslinked multifunctional hydrogel for diabetic wound healing. Compos Part B Eng 2023; 257:110687. doi: 10.1016/j.compositesb.2023.110687 [Crossref] [ Google Scholar]
- Wang Y, Zhai W, Cheng S, Li J, Zhang H. Surface-functionalized design of blood-contacting biomaterials for preventing coagulation and promoting hemostasis. Friction 2023; 11:1371-94. doi: 10.1007/s40544-022-0710-x [Crossref] [ Google Scholar]
- He W, Wang Y, Li X, Ji Y, Yuan J, Yang W. Sealing the Pandora’s vase of pancreatic fistula through entrapping the digestive enzymes within a dextrorotary (D)-peptide hydrogel. Nat Commun 2024; 15:7235. doi: 10.1038/s41467-024-51734-7 [Crossref] [ Google Scholar]
- Xu L, Zhang J, Luo J, Cui Y, Chen J, Zeng B. “Double-sided protector” Janus hydrogels for skin and mucosal wound repair: applications, mechanisms, and prospects. J Nanobiotechnol 2025; 23:387. doi: 10.1186/s12951-025-03438-3 [Crossref] [ Google Scholar]
- Singh S, Syukri DM, Ushir YV, Mishra A, Ontong JC, Nwabor OF. Post-operative Wound Healing Efficacy of Eucalyptus Camaldulensis Phenolic-rich Extracts Incorporated Hydrogel With Enhanced Antioxidant, Antibacterial, and Anti-inflammatory Activities. J Polym Environ 2025; 33:814-39. doi: 10.1007/s10924-024-03427-x [Crossref] [ Google Scholar]
- Khamkat P, Barik V, Mohapatra S, Karati D, Mukherjee S. Current Approaches on Transfersomal Patch: A Noninvasive Innovative Booster for Improved Transdermal Drug Delivery. Curr Pharm Biotechnol 2025; 26:2127-2140. doi: 10.2174/0113892010315069240805074205 [Crossref] [ Google Scholar]
-
Huang B, An H, Chu J, Ke S, Ke J, Qiu Y, et al. Glucose-Responsive and Analgesic Gel for Diabetic Subcutaneous Abscess Treatment by Simultaneously Boosting Photodynamic Therapy and Relieving Hypoxia. Adv Sci (Weinh) 2025; e02830. doi: 10.1002/advs.202502830.
- Kabashima K, Honda T, Ginhoux F, Egawa G. The immunological anatomy of the skin. Nat Rev Immunol 2019; 19:19-30. doi: 10.1038/s41577-018-0084-5 [Crossref] [ Google Scholar]
- Tai Q-D, Tang Y, Xie S-T, Ye Y-Y, Tang X, Lyu Q. Glucose-responsive nanozyme hydrogel for glycemic control and catalytic anti-infective therapy in diabetic wound healing. Mater Today Bio 2025; 35:102405. doi: 10.1016/j.mtbio.2025.102405 [Crossref] [ Google Scholar]
- Ye Y, Liu Y, Ma S, Li X, Wang W, Chen X. Multifunctional DNA hydrogels with light-triggered gas-therapy and controlled G-Exos release for infected wound healing. Bioact Mater 2025; 52:422-37. doi: 10.1016/j.bioactmat.2025.06.004 [Crossref] [ Google Scholar]
- Mishra T, Verma S, Verma VS, Mishra A, Jeswani G, Sahu D. In-silico molecular docking and screening of Costus specious bioactive compounds as potential herb in management of diabetes mellitus. Vegetos 2025; 38:2319-32. doi: 10.1007/s42535-024-01034-8 [Crossref] [ Google Scholar]
- Akkus G, Sert M. Diabetic foot ulcers: A devastating complication of diabetes mellitus continues non-stop in spite of new medical treatment modalities. World J Diabetes 2022; 13:1106. doi: 10.4239/wjd.v13.i12.1106 [Crossref] [ Google Scholar]
- Liang J, He Y, Huang C, Ji F, Zhou X, Yin Y. The Regulation of Selenoproteins in Diabetes: A New Way to Treat Diabetes. Curr Pharm Des 2024; 30:1541-7. doi: 10.2174/0113816128302667240422110226 [Crossref] [ Google Scholar]
- Raja JM, Maturana MA, Kayali S, Khouzam A, Efeovbokhan N. Diabetic foot ulcer: A comprehensive review of pathophysiology and management modalities. World J Clin Cases 2023; 11:1684. doi: 10.12998/wjcc.v11.i8.1684 [Crossref] [ Google Scholar]
-
Mohite P, Puri A, Pandhare R, Singh S, Sonawane M, Pawar A. Biomaterials-Based Additive Manufactured Products for Chronic Wound Healing. In: Singh S, P Mohite, D Datta, editors. Biomaterial-based Additive Manufacturing in Tissue Engineering and Regeneration. Cham: Springer Nature Switzerland; 2025. p. 253-78. doi: 10.1007/978-3-031-96070-3_9.
- McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care 2023; 46:209-21. doi: 10.2337/dci22-0043 [Crossref] [ Google Scholar]
- Wang W, Cai T, Shao C, Xiao Y, Xiang Y, Jiang Y. MXene-Based Responsive Hydrogels and Applications in Wound Healing. Chemistry Select 2024; 9:e202402073. doi: 10.1002/slct.202402073 [Crossref] [ Google Scholar]
- Pereira MG, Vilaça M, Pedras S, Carvalho A, Vedhara K, Dantas MJ. Wound healing and healing process in patients with diabetic foot ulcers: A survival analysis study. Diabetes Res Clin Pract 2023; 198:110623. doi: 10.1016/j.diabres.2023.110623 [Crossref] [ Google Scholar]
- Nirenjen S, Narayanan J, Tamilanban T, Subramaniyan V, Chitra V, Fuloria NK. Exploring the contribution of pro-inflammatory cytokines to impaired wound healing in diabetes. Front Immunol 2023; 14:1216321. doi: 10.3389/fimmu.2023.1216321 [Crossref] [ Google Scholar]
- Baltzis D, Eleftheriadou I, Veves A. Pathogenesis and treatment of impaired wound healing in diabetes mellitus: new insights. Adv Ther 2014; 31:817-36. doi: 10.1007/s12325-014-0140-x [Crossref] [ Google Scholar]
-
Dasari N, Jiang A, Skochdopole A, Chung J, Reece EM, Vorstenbosch J, et al, editors. Updates in diabetic wound healing, inflammation, and scarring. Thieme Medical Publishers, Inc; 2021. doi: 10.1055/s-0041-1731460.
- Uchida DT, Bruschi ML. 3D printing as a technological strategy for the personalized treatment of wound healing. AAPS PharmSciTech 2023; 24:41. doi: 10.1208/s12249-023-02503-0 [Crossref] [ Google Scholar]
-
Abisatya AMA, Mutiadesi WP, Purwaningsari D, Yudadi R, Adiwinoto RP. The effect of type 2 diabetes mellitus (T2DM) as a comorbid factor on the morbidity rate and length of hospital stay (LoS) in patients undergoing cholecystectomy: T2DM as comorbid factor affecting morbidity and LoS in cholecystectomic. Surabaya Med J 2024; 14-21. doi: 10.59747/smjidisurabaya.v2i1.49.
- Holl J, Kowalewski C, Zimek Z, Fiedor P, Kaminski A, Oldak T. Chronic diabetic wounds and their treatment with skin substitutes. Cells 2021; 10:655. doi: 10.3390/cells10030655 [Crossref] [ Google Scholar]
- Carnaby-Mann G, Crary M. Pill swallowing by adults with dysphagia. Arch Otolaryngol Head Neck Surg 2005; 131:970-5. doi: 10.1001/archotol.131.11.970 [Crossref] [ Google Scholar]
- Xu F, Rui S, Yang C, Jiang X, Wu W, Tang X. Bioprinting technology for the management of diabetic foot disease: Emerging applications, challenges, and prospects. Int J Bioprinting 2023; 9:0142. doi: 10.36922/ijb.0142 [Crossref] [ Google Scholar]
- Vyas J, Raytthatha N, Vyas P, Prajapati BG, Uttayarat P, Singh S. Biomaterial-Based Additive Manufactured Composite/Scaffolds for Tissue Engineering and Regenerative Medicine: A Comprehensive Review. Polymers 2025; 17:1090. doi: 10.3390/polym17081090 [Crossref] [ Google Scholar]
- Li X, Ai X, Wang B, Luo M, Miyamoto A, Kuchay MS. Application of 3D printing in the treatment of diabetic foot ulcers: current status and new insights. Front Bioeng Biotechnol 2024; 12:1475885. doi: 10.3389/fbioe.2024.1475885 [Crossref] [ Google Scholar]
- Patel P, Garala K, Singh S, Prajapati BG, Chittasupho C. Lipid-Based Nanoparticles in Delivering Bioactive Compounds for Improving Therapeutic Efficacy. Pharmaceuticals 2024; 17:329. doi: 10.3390/ph17030329 [Crossref] [ Google Scholar]
- Singh S, Supaweera N, Nwabor OF, Chaichompoo W, Suksamrarn A, Chittasupho C. Poly (vinyl alcohol)-gelatin-sericin copolymerized film fortified with vesicle-entrapped demethoxycurcumin/bisdemethoxycurcumin for improved stability, antibacterial, anti-inflammatory, and skin tissue regeneration. Int J Biol Macromol 2024; 258:129071. doi: 10.1016/j.ijbiomac.2023.129071 [Crossref] [ Google Scholar]
- Jayeoye TJ, Eze FN, Singh S, Olatunde OO, Benjakul S, Rujiralai T. Synthesis of gold nanoparticles/polyaniline boronic acid/sodium alginate aqueous nanocomposite based on chemical oxidative polymerization for biological applications. Int J Biol Macromol 2021; 179:196-205. doi: 10.1016/j.ijbiomac.2021.02.199 [Crossref] [ Google Scholar]
- Singh S, Nwabor OF, Sukri DM, Wunnoo S, Dumjun K, Lethongkam S. Poly (vinyl alcohol) copolymerized with xanthan gum/hypromellose/sodium carboxymethyl cellulose dermal dressings functionalized with biogenic nanostructured materials for antibacterial and wound healing application. Int J Biol Macromol 2022; 216:235-50. doi: 10.1016/j.ijbiomac.2022.06.172 [Crossref] [ Google Scholar]
- Vyas J, Singh S, Shah I, Prajapati BG. Potential Applications and Additive Manufacturing Technology-Based Considerations of Mesoporous Silica: A Review. AAPS PharmSciTech 2023; 25:6. doi: 10.1208/s12249-023-02720-7 [Crossref] [ Google Scholar]
- Calignano F, Manfredi D, Ambrosio EP, Biamino S, Lombardi M, Atzeni E. Overview on additive manufacturing technologies. Proc IEEE 2017; 105:593-612. doi: 10.1109/JPROC.2016.2625098 [Crossref] [ Google Scholar]
- Petrovic V, Vicente Haro Gonzalez J, Jordá Ferrando O, Delgado Gordillo J, Ramón Blasco Puchades J, Portolés Griñan L. Additive layered manufacturing: sectors of industrial application shown through case studies. Int J Prod Res 2011; 49:1061-79. doi: 10.1080/00207540903479786 [Crossref] [ Google Scholar]
- Motealleh A, Çelebi-Saltik B, Ermis N, Nowak S, Khademhosseini A, Kehr NS. 3D printing of step-gradient nanocomposite hydrogels for controlled cell migration. Biofabrication 2019; 11:045015. doi: 10.1088/1758-5090/ab3582 [Crossref] [ Google Scholar]
- Mohite P, Asane G, Rebello N, Munde S, Ade N, Boban T. Polymeric Hydrogel Sponges for Wound Healing Applications: A Comprehensive Review. Regen Eng Transl Med 2024; 10:416-37. doi: 10.1007/s40883-024-00334-4 [Crossref] [ Google Scholar]
- Bose S, Ke D, Sahasrabudhe H, Bandyopadhyay A. Additive manufacturing of biomaterials. Prog Mater Sci 2018; 93:45-111. doi: 10.1016/j.pmatsci.2017.08.003 [Crossref] [ Google Scholar]
- Wu Y, Lu Y, Zhao M, Bosiakov S, Li L. A critical review of additive manufacturing techniques and associated biomaterials used in bone tissue engineering. Polymers 2022; 14:2117. doi: 10.3390/polym14102117 [Crossref] [ Google Scholar]
- Mironov V, Visconti RP, Kasyanov V, Forgacs G, Drake CJ, Markwald RR. Organ printing: tissue spheroids as building blocks. Biomaterials 2009; 30:2164-74. doi: 10.1016/j.biomaterials.2008.12.084 [Crossref] [ Google Scholar]
- Zhao X, Hu DA, Wu D, He F, Wang H, Huang L. Applications of biocompatible scaffold materials in stem cell-based cartilage tissue engineering. Front Bioeng Biotechnol 2021; 9:603444. doi: 10.3389/fbioe.2021.603444 [Crossref] [ Google Scholar]
- Boland T, Tao X, Damon BJ, Manley B, Kesari P, Jalota S. Drop-on-demand printing of cells and materials for designer tissue constructs. Mater Sci Eng C 2007; 27:372-6. doi: 10.1016/j.msec.2006.05.047 [Crossref] [ Google Scholar]
- Gudapati H, Dey M, Ozbolat I. A comprehensive review on droplet-based bioprinting: Past, present and future. Biomaterials 2016; 102:20-42. doi: 10.1016/j.biomaterials.2016.06.012 [Crossref] [ Google Scholar]
- Jamee R, Araf Y, Naser IB, Promon SK. The promising rise of bioprinting in revolutionalizing medical science: Advances and possibilities. Regen Ther 2021; 18:133-45. doi: 10.1016/j.reth.2021.05.006 [Crossref] [ Google Scholar]
- Umur E, Bayrak E, Arslan F, Bulut SB, Baysoy E, Kaleli-Can G. Advances in three dimensional bioprinting for wound healing: a comprehensive review. Appl Sci (Basel) 2023; 13:10269. doi: 10.3390/app131810269 [Crossref] [ Google Scholar]
- Velema J, Kaplan D. Biopolymer-based biomaterials as scaffolds for tissue engineering. Adv Biochem Eng Biotechnol 2006; 102:187-238. doi: 10.1007/10_013 [Crossref] [ Google Scholar]
- Hutmacher DW, Sittinger M, Risbud MV. Scaffold-based tissue engineering: rationale for computer-aided design and solid free-form fabrication systems. Trends Biotechnol 2004; 22:354-62. doi: 10.1016/j.tibtech.2004.05.005 [Crossref] [ Google Scholar]
- Melchels FPW, Feijen J, Grijpma DW. A review on stereolithography and its applications in biomedical engineering. Biomaterials 2010; 31:6121-30. doi: 10.1016/j.biomaterials.2010.04.050 [Crossref] [ Google Scholar]
- Hsieh TM, Ng CWB, Narayanan K, Wan ACA, Ying JY. Three-dimensional microstructured tissue scaffolds fabricated by two-photon laser scanning photolithography. Biomaterials 2010; 31:7648-52. doi: 10.1016/j.biomaterials.2010.06.029 [Crossref] [ Google Scholar]
- Lin H, Zhang D, Alexander PG, Yang G, Tan J, Cheng AW-M. Application of visible light-based projection stereolithography for live cell-scaffold fabrication with designed architecture. Biomaterials 2013; 34:331-9. doi: 10.1016/j.biomaterials.2012.09.048 [Crossref] [ Google Scholar]
- Dickinson LE, Gerecht S. Engineered biopolymeric scaffolds for chronic wound healing. Front Physiol 2016; 7:341. doi: 10.3389/fphys.2016.00341 [Crossref] [ Google Scholar]
- Tallapaneni V, Kalaivani C, Pamu D, Mude L, Singh SK, Karri VVSR. Acellular scaffolds as innovative biomaterial platforms for the management of diabetic wounds. Tissue Eng Regen Med 2021; 18:713-34. doi: 10.1007/s13770-021-00344-1 [Crossref] [ Google Scholar]
- Damiri F, Fatimi A, Magdalena Musuc A, Paiva Santos AC, Paszkiewicz S, Igwe Idumah C. Nano-hydroxyapatite (nHAp) scaffolds for bone regeneration: Preparation, characterization and biological applications. J Drug Deliv Sci Technol 2024; 95:105601. doi: 10.1016/j.jddst.2024.105601 [Crossref] [ Google Scholar]
-
Singh A, Mandal P, Maheshwari S, Akhtar J, Prajapati BG, Singh S. Processing of Sustainable Biomaterials by Additive Manufacturing Methods. In: Advances in Sustainable Biomaterials. CRC Press; 2024. p. 141-62. doi: 10.1201/9781003434313.
- Zohdi N, Yang R. Material anisotropy in additively manufactured polymers and polymer composites: a review. Polymers 2021; 13:3368. doi: 10.3390/polym13193368 [Crossref] [ Google Scholar]
- Antezana PE, Municoy S, Álvarez-Echazú MI, Santo-Orihuela PL, Catalano PN, Al-Tel TH. The 3D bioprinted scaffolds for wound healing. Pharmaceutics 2022; 14:464. doi: 10.3390/pharmaceutics14020464 [Crossref] [ Google Scholar]
- Galvão Duarte J, Piedade AP, Sarmento B, Mascarenhas‐Melo F. The Printed Path to Healing: Advancing Wound Dressings through Additive Manufacturing. Adv Healthc Mater 2025; 14:2402711. doi: 10.1002/adhm.202402711 [Crossref] [ Google Scholar]
- Schneider J, Kumar S. Multiscale characterization and constitutive parameters identification of polyamide (PA12) processed via selective laser sintering. Polym Test 2020; 86:106357. doi: 10.1016/j.polymertesting.2020.106357 [Crossref] [ Google Scholar]
- Tiwari SK, Pande S, Agrawal S, Bobade SM. Selection of selective laser sintering materials for different applications. Rapid Prototyp J 2015; 21:630-48. doi: 10.1108/RPJ-03-2013-0027 [Crossref] [ Google Scholar]
- Ren Y, Wang H, Song X, Wu Y, Lyu Y, Zeng W. Advancements in diabetic foot insoles: a comprehensive review of design, manufacturing, and performance evaluation. Front Bioeng Biotechnol 2024; 12:1394758. doi: 10.3389/fbioe.2024.1394758 [Crossref] [ Google Scholar]
- Chhikara K, Singh G, Gupta S, Chanda A. Progress of additive manufacturing in fabrication of foot orthoses for diabetic patients: a review. Ann 3D Print Med 2022; 8:100085. doi: 10.1016/j.stlm.2022.100085 [Crossref] [ Google Scholar]
- Kundumani Janarthanan AK, Vaidhyanathan B. Additive Manufacturing of Smart Footwear Components for Healthcare Applications. Micromachines 2024; 16:30. doi: 10.3390/mi16010030 [Crossref] [ Google Scholar]
-
Chen T, Tian M, Wang X, editors. A novel porous structural design of the orthotic insole for diabetic foot. IEEE; 2021. doi: 10.1109/ICCCR49711.2021.9349389.
- De Pascali C, Francioso L, Giampetruzzi L, Rescio G, Signore MA, Leone A. Modeling, fabrication and integration of wearable smart sensors in a monitoring platform for diabetic patients. Sensors 2021; 21:1847. doi: 10.3390/s21051847 [Crossref] [ Google Scholar]
- Ning L, Chen X. A brief review of extrusion‐based tissue scaffold bio‐printing. Biotechnol J 2017; 12:1600671. doi: 10.1002/biot.201600671 [Crossref] [ Google Scholar]
- Armstrong AA, Pfeil A, Alleyne AG, Johnson AJW. Process monitoring and control strategies in extrusion-based bioprinting to fabricate spatially graded structures. Bioprinting 2021; 21:e00126. doi: 10.1016/j.bprint.2020.e00126 [Crossref] [ Google Scholar]
- Lee VK, Lanzi AM, Ngo H, Yoo S-S, Vincent PA, Dai G. Generation of multi-scale vascular network system within 3D hydrogel using 3D bio-printing technology. Cell Mol Bioeng 2014; 7:460-72. doi: 10.1007/s12195-014-0340-0 [Crossref] [ Google Scholar]
- Shah SR, Modi CD, Singh S, Mori DD, Soniwala MM, Prajapati BG. Recent Advances in Additive Manufacturing of Polycaprolactone-Based Scaffolds for Tissue Engineering Applications: A Comprehensive Review. Regen Eng Transl Med 2025; 11:112-31. doi: 10.1007/s40883-024-00351-3 [Crossref] [ Google Scholar]
- Puppi D, Piras AM, Pirosa A, Sandreschi S, Chiellini F. Levofloxacin-loaded star poly (ε-caprolactone) scaffolds by additive manufacturing. J Mater Sci Mater Med 2016; 27:44. doi: 10.1007/s10856-015-5658-1 [Crossref] [ Google Scholar]
- Sánchez-González S, Diban N, Urtiaga A. Hydrolytic degradation and mechanical stability of poly (ε-Caprolactone)/reduced graphene oxide membranes as scaffolds for in vitro neural tissue regeneration. Membranes 2018; 8:12. doi: 10.3390/membranes8010012 [Crossref] [ Google Scholar]
- Ramesh S, Harrysson OLA, Rao PK, Tamayol A, Cormier DR, Zhang Y. Extrusion bioprinting: Recent progress, challenges, and future opportunities. Bioprinting 2021; 21:e00116. doi: 10.1016/j.bprint.2020.e00116 [Crossref] [ Google Scholar]
- Sathisaran I. 3D printing and bioprinting in the battle against diabetes and its chronic complications. Front Bioeng Biotechnol 2024; 12:1363483. doi: 10.3389/fbioe.2024.1363483 [Crossref] [ Google Scholar]
- Lozano R, Stevens L, Thompson BC, Gilmore KJ, Gorkin Iii R, Stewart EM. 3D printing of layered brain-like structures using peptide modified gellan gum substrates. Biomaterials 2015; 67:264-73. doi: 10.1016/j.biomaterials.2015.07.022 [Crossref] [ Google Scholar]
- Mohite P, Puri A, Munde S, Dave R, Khan S, Patil R. Potential of Chitosan/Gelatin-Based Nanofibers in Delivering Drugs for the Management of Varied Complications: A Review. Polymers 2025; 17:435. doi: 10.3390/polym17040435 [Crossref] [ Google Scholar]
-
Basu B, Mallick S, Dhauria S, Nagime PV, Singh S. Native/modified dextran-based nanogel in delivering drug and management of ocular complications: a review. Z Naturforsch C 2025; 81(1-2). doi: 10.1515/znc-2025-0014.
- Gungor-Ozkerim PS, Inci I, Zhang YS, Khademhosseini A, Dokmeci MR. Bioinks for 3D bioprinting: an overview. Biomater Sci 2018; 6:915-46. [ Google Scholar]
- Levato R, Visser J, Planell JA, Engel E, Malda J, Mateos-Timoneda MA. Biofabrication of tissue constructs by 3D bioprinting of cell-laden microcarriers. Biofabrication 2014; 6:035020. doi: 10.1039/c7bm00765e [Crossref] [ Google Scholar]
- Buyukhatipoglu K, Jo W, Sun W, Clyne AM. The role of printing parameters and scaffold biopolymer properties in the efficacy of a new hybrid nano-bioprinting system. Biofabrication 2009; 1:035003. doi: 10.1088/1758-5082/1/3/035003 [Crossref] [ Google Scholar]
- Jang J-W, Min K-E, Kim C, Wern C, Yi S. Rheological properties and 3D printing behavior of PCL and DMSO2 composites for bio-scaffold. Materials 2024; 17:2459. doi: 10.3390/ma17102459 [Crossref] [ Google Scholar]
- Balaji KV, Bhutoria S, Nayak S, Kumar PRA, Velayudhan S. Printability assessment of modified filament deposition modelling three dimensional bioprinter printer using polymeric formulations. Biomed Eng Adv 2023; 5:100083. doi: 10.1016/j.bea.2023.100083 [Crossref] [ Google Scholar]
- Sedlak J, Joska Z, Jansky J, Zouhar J, Kolomy S, Slany M. Analysis of the mechanical properties of 3D-printed plastic samples subjected to selected degradation effects. Materials 2023; 16:3268. doi: 10.3390/ma16083268 [Crossref] [ Google Scholar]
- Hu Y, Wu B, Xiong Y, Tao R, Panayi AC, Chen L. Cryogenic 3D printed hydrogel scaffolds loading exosomes accelerate diabetic wound healing. Chem Eng J 2021; 426:130634. doi: 10.1016/j.cej.2021.130634 [Crossref] [ Google Scholar]
- Lin Z, Xie W, Cui Z, Huang J, Cao H, Li Y. 3D printed alginate/gelatin-based porous hydrogel scaffolds to improve diabetic wound healing. Giant 2023; 16:100185. doi: 10.1016/j.giant.2023.100185 [Crossref] [ Google Scholar]
- Chen B, Dong J, Ruelas M, Ye X, He J, Yao R. Artificial intelligence‐assisted high‐throughput screening of printing conditions of hydrogel architectures for accelerated diabetic wound healing. Adv Funct Mater 2022; 32:2201843. doi: 10.1002/adfm.202201843 [Crossref] [ Google Scholar]
- Kim N, Lee H, Han G, Kang M, Park S, Kim DE. 3D‐Printed functional hydrogel by DNA‐induced biomineralization for accelerated diabetic wound healing. Adv Sci 2023; 10:2300816. doi: 10.1002/advs.202300816 [Crossref] [ Google Scholar]
- Li S, Xu Y, Zheng L, Fan C, Luo F, Zou Y. High self‐supporting chitosan‐based hydrogel ink for in situ 3D printed diabetic wound dressing. Adv Funct Mater 2025; 35:2414625. doi: 10.1002/adfm.202414625 [Crossref] [ Google Scholar]
-
Alaa AL, Yehia S, Sayed HAE, Hussein MAM, El-Sayed E-SM, El-Sherbiny IM. Multifunctional bilayer wound dressing based on 3D-printed sodium alginate/gelatin hydrogel and polycaprolactone nanofibers for accelerating diabetic wound healing. Int J Biol Macromol 2025; 144832. doi: 10.1016/j.ijbiomac.2025.144832.
- Naik K, Singh P, Yadav M, Srivastava SK, Tripathi S, Ranjan R. 3D printable, injectable amyloid-based composite hydrogel of bovine serum albumin and aloe vera for rapid diabetic wound healing. J Mater Chem B 2023; 11:8142-58. doi: 10.1039/D3TB01151H [Crossref] [ Google Scholar]
- Yang H, Wang Y, Li R, Shen Y-F, Zhou F-F, Tan W-Q. A 3D-printed grid-like hyaluronic acid based hydrogel loaded with deferoxamine as wound dressing promotes diabetic wound healing. Int J Biol Macromol 2025; 303:140598. doi: 10.1016/j.ijbiomac.2025.140598 [Crossref] [ Google Scholar]
- Guo L, Niu X, Chen X, Lu F, Gao J, Chang Q. 3D direct writing egg white hydrogel promotes diabetic chronic wound healing via self-relied bioactive property. Biomaterials 2022; 282:121406. doi: 10.1016/j.biomaterials.2022.121406 [Crossref] [ Google Scholar]
- Cao W, Peng S, Yao Y, Xie J, Li S, Tu C. A nanofibrous membrane loaded with doxycycline and printed with conductive hydrogel strips promotes diabetic wound healing in vivo. Acta biomaterialia 2022; 152:60-73. doi: 10.1016/j.actbio.2022.08.048 [Crossref] [ Google Scholar]
- Ding X, Yu Y, Li W, Zhao Y. In situ 3D-bioprinting MoS2 accelerated gelling hydrogel scaffold for promoting chronic diabetic wound healing. Matter 2023; 6:1000-14. doi: 10.1016/j.matt.2023.01.001 [Crossref] [ Google Scholar]
- Liu H, Nail A, Meng D, Zhu L, Guo X, Li C. 3D printed eutectogel dissolving microneedles patch loaded with chitosan-based nanoparticles for diabetic wound management. Int J Biol Macromol 2025; 307:142018. doi: 10.1016/j.ijbiomac.2025.142018 [Crossref] [ Google Scholar]
- Lihao Q, Tingting L, Jiawei Z, Yifei B, Zheyu T, Jingyan L. 3D bioprinting of Salvianolic acid B-sodium alginate-gelatin skin scaffolds promotes diabetic wound repair via antioxidant, anti-inflammatory, and proangiogenic effects. Biomed Pharmacother 2024; 171:116168. doi: 10.1016/j.biopha.2024.116168 [Crossref] [ Google Scholar]
- Wang X, Zhang Y, Song A, Wang H, Wu Y, Chang W. A printable hydrogel loaded with medicinal plant extract for promoting wound healing. Adv Healthc Mater 2024; 13:2303017. doi: 10.1002/adhm.202303017 [Crossref] [ Google Scholar]
- Piva HL, de Queiroz MS, Matsuo FS, Borges HS, Osako MK, Tedesco AC. StemCurCol–3D Printed scaffold for diabetic wound regeneration. Ann 3D Print Med 2025; 18:100203. doi: 10.1016/j.stlm.2025.100203 [Crossref] [ Google Scholar]
- Wan W, Cai F, Huang J, Chen S, Liao Q. A skin-inspired 3D bilayer scaffold enhances granulation tissue formation and anti-infection for diabetic wound healing. J Mater Chem B 2019; 7:2954-61. doi: 10.1039/C8TB03341B [Crossref] [ Google Scholar]
- Lonardi R, Leone N, Gennai S, Trevisi Borsari G, Covic T, Silingardi R. Autologous micro-fragmented adipose tissue for the treatment of diabetic foot minor amputations: a randomized controlled single-center clinical trial (MiFrAADiF). Stem Cell Res Ther 2019; 10:223. doi: 10.1186/s13287-019-1328-4 [Crossref] [ Google Scholar]
- Armstrong DG, Harris SG, Rasor Z, Zelen CM, Kim J, Swerdlow M. Autologous minimally manipulated homologous adipose tissue (AMHAT) for treatment of nonhealing diabetic foot ulcers. PRS Global Open 2022; 10:e4588. doi: 10.1097/gox.0000000000004588 [Crossref] [ Google Scholar]
- Kesavan R, Sheela Sasikumar C, Narayanamurthy VB, Rajagopalan A, Kim J. Management of diabetic foot ulcer with MA–ECM (minimally manipulated autologous extracellular matrix) using 3D bioprinting technology–an innovative approach. Int J Low Extrem Wounds 2024; 23:161-8. doi: 10.1177/15347346211045625 [Crossref] [ Google Scholar]
- Bajuri MY, Kim J, Yu Y, Shahul Hameed MS. New paradigm in diabetic foot ulcer grafting techniques using 3D-bioprinted autologous minimally manipulated homologous adipose tissue (3D-AMHAT) with fibrin gel acting as a biodegradable scaffold. Gels 2023; 9:66. doi: 10.3390/gels9010066 [Crossref] [ Google Scholar]
- Zaszczyńska A, Moczulska-Heljak M, Gradys A, Sajkiewicz P. Advances in 3D printing for tissue engineering. Materials 2021; 14:3149. doi: 10.3390/ma14123149 [Crossref] [ Google Scholar]
- Tsakmaki A, Fonseca Pedro P, Bewick GA. Diabetes through a 3D lens: organoid models. Diabetologia 2020; 63:1093-102. doi: 10.1007/s00125-020-05126-3 [Crossref] [ Google Scholar]
- Choudhury S, Dhoke NR, Chawla S, Das A. Bioengineered MSC Cxcr2 transdifferentiated keratinocyte-like cell-derived organoid potentiates skin regeneration through ERK1/2 and STAT3 signaling in diabetic wound. Cell Mol Life Sci 2024; 81:172. doi: 10.1007/s00018-023-05057-3 [Crossref] [ Google Scholar]
- Mathur V, Agarwal P, Kasturi M, Srinivasan V, Seetharam RN, Vasanthan KS. Innovative bioinks for 3D bioprinting: Exploring technological potential and regulatory challenges. J Tissue Eng 2025; 16:20417314241308022. doi: 10.1177/20417314241308022 [Crossref] [ Google Scholar]
- Zoghi S. Advancements in tissue engineering: A review of bioprinting techniques, scaffolds, and bioinks. Biomed Eng Comput Biol 2024; 15:11795972241288099. doi: 10.1177/11795972241288099 [Crossref] [ Google Scholar]
- Singh S, Chunglok W, Nwabor OF, Chulrik W, Jansakun C, Bhoopong P. Porous Biodegradable Sodium Alginate Composite Fortified with Hibiscus Sabdariffa L Calyx Extract for the Multifarious Biological Applications and Extension of Climacteric Fruit Shelf-Life. J Polym Environ 2023; 31:922-38. doi: 10.1007/s10924-022-02596-x [Crossref] [ Google Scholar]
- Basu B, Rahaman M, Ghosh S, Dutta S, Kumar A, Mukherjee S. Emerging silk sericin-based formulation fortified with therapeutics in the management of diabetic wound and skin tissue regeneration. Z Naturforsch C J Biosci 2025; 80:597-626. doi: 10.1515/znc-2024-0198 [Crossref] [ Google Scholar]
- Tabriz AG, Douroumis D. Recent advances in 3D printing for wound healing: A systematic review. J Drug Deliv Sci Technol 2022; 74:103564. doi: 10.1016/j.jddst.2022.103564 [Crossref] [ Google Scholar]
- Fawzy A, Benaziria I. Reviewing Advances in Skin Grafting for Diabetic Foot Ulcers. IJMSCRS 2023; 3:1874-84. doi: 10.47191/ijmscrs/v3-i9-14 [Crossref] [ Google Scholar]
- Ng WL, An J, Chua CK. Process, material, and regulatory considerations for 3D printed medical devices and tissue constructs. Engineering 2024; 36:146-66. doi: 10.1016/j.eng.2024.01.028 [Crossref] [ Google Scholar]
-
Co JRM, Culaba AB, editors. 3D printing: challenges and opportunities of an emerging disruptive technology. IEEE; 2019. doi: 10.1109/HNICEM48295.2019.9073427.
- Wang D, Zhang J, Liu Q, Chen B, Liang Y, Hu L. 3D printing challenges in enabling rapid response to public health emergencies. Innovation (Camb) 2020; 1:100056. doi: 10.1016/j.xinn.2020.100056 [Crossref] [ Google Scholar]
- Ojeh N, Pastar I, Tomic-Canic M, Stojadinovic O. Stem cells in skin regeneration, wound healing, and their clinical applications. Int J Mol Sci 2015; 16:25476-501. doi: 10.3390/ijms161025476 [Crossref] [ Google Scholar]
- Shopova D, Yaneva A, Bakova D, Mihaylova A, Kasnakova P, Hristozova M. (Bio) printing in personalized medicine—opportunities and potential benefits. Bioengineering 2023; 10:287. doi: 10.3390/bioengineering10030287 [Crossref] [ Google Scholar]
- Kothawade S, Singh S. Recent Advancements in Stimuli-Responsive Polymeric Implants Fabricated via Additive Manufacturing: A Review. Curr Pharm Des 2026; 32:12-35. doi: 10.2174/0113816128368347250515073105 [Crossref] [ Google Scholar]
- Ahmed A, Arya S, Gupta V, Furukawa H, Khosla A. 4D printing: Fundamentals, materials, applications and challenges. Polymer 2021; 228:123926. doi: 10.1016/j.polymer.2021.123926 [Crossref] [ Google Scholar]